Download
1 / 14
140 likes | 304 Views
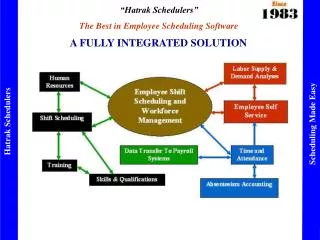
HIV/STD Surveillance in Tennessee: A fully integrated model. Thomas J. Shavor, MBA, MPH Epidemiology Director HIV/STD Surveillance & Data Management Tennessee Department of Health. Surveillance Integration in Tennessee.

E N D
HIV/STD Surveillance in Tennessee: A fully integrated model Thomas J. Shavor, MBA, MPH Epidemiology Director HIV/STD Surveillance & Data Management Tennessee Department of Health
Surveillance Integration in Tennessee • Definition- Combining all aspects of HIV/STD surveillance activities in order to attain a close and seamless coordination of information/services between: • Groups within HIV/STD Surveillance & Data Management (Group Level Integration) • Program areas within HIV/STD Section (Program Level Integration)
Tennessee: a short snapshot • 2007 Population: 6,054,830 (Source: U.S. Census) • Approx. 1,000 new HIV/AIDS diagnoses/year (Source: Tennessee HARS) • 13,521 living with HIV/AIDS as of 12/31/06 (Source: Tennessee HARS) • High historical STD rates (Source 2005 CDC STD Surveillance Report) • 8th highest rates of Chlamydia • 13th highest rates of Gonorrhea • 10th highest rates of P&S Syphilis
Brief Historical Timeline • 1982- Tennessee began collecting AIDS case data • 1986- Tennessee established an AIDS program within the Bureau of Health Services • 1987- AIDS reporting becomes mandatory • 1992- HIV reporting becomes mandatory • 2001- The STD Prevention, HIV Prevention, and Ryan White programs merged to become the HIV/STD Section • 2003- Current organization finalized
Levels of Integration • Integration occurs at 2 levels: • Surveillance level- Core, Incidence, CTS, PEMS (?), Behavioral Surveillance, STD Surveillance, Chlamydia Infertility, and Program Evaluation groups occur within a single unit (housed in a secure area within our section) 2. Program level- HIV/AIDS/STD Surveillance section is integrated with the HIV/STD Prevention, Ryan White, and IT Support programs within the section.
Surveillance & Data Management Ryan White Program HIV/STD Prevention Program Program Level Integration
Surveillance Position Funding Sources • Epidemiology Director-100% HIV Core Surveillance • Prevention Epidemiologist- funded 50% by HIV Prevention/50% by STD Prevention • STD Public Health Advisor (2)-100% STD Prevention • HIV Epidemiologist-90% EpiTA/10% Core Surveillance • Ryan White Epidemiologist- 100% Ryan White Program • HIV Surveillance Reps (10)- 10%-100% HIV Core Surveillance (depending on area) • Clerical Support/ICCR(2)-100% STD Prevention
HIV/STD Surveillance Activities • Responsible for providing data for ALL grants, including: • HIV Surveillance • STD Prevention • HIV Prevention • HIV Counseling/Testing • Ryan White (Part A and Part B) • Chlamydia Infertility • Maternal Child Health, TB, and anyone else
HIV/STD Surveillance Activities-cont. • Manage and analyze data from a variety of databases: • HARS/eHARS • STD*MIS • PTBMIS (Tennessee’s Patient billing system) • PEMS (???) • Ryan White Care-Ware • Chlamydia Infertility database • Joint datasets (HIV Unmet Need, etc.)
Benefits of Integration • Allows for more effective communication within Surveillance groups & between different programs • Helps program staff to see the “big picture” • Has potential to save time (fewer meetings) • Encourages each program area to participate in collaborative projects • Aids in resource planning for future needs • Assists in program evaluation activities
Challenges of Integration • Cross-training surveillance staff (i.e. “doing more with less”) to perform unfamiliar tasks can lead to major stress! • Managers must attain a greater understanding of how other program areas function. • Breaking down traditional program barriers can be difficult (“my program-your program”) • Explaining “technical” subjects to non-technical people can be frustrating! • Getting programs to pay their “fair share” of Surveillance resources used
Integration: Skills needed for success • Organize time/materials/resources • Learning skills outside of your comfort zone • Ensure lines of communication are always open (via regularly scheduled management meetings) • Involve others in grant preparation, program evaluation, routine decisions • PATIENCE!