Download

1 / 28
280 likes | 339 Views
This workshop covers the dosing considerations for drug therapy in obese children, focusing on body composition, physiological changes in obesity, pharmacokinetic parameter changes, clinical evidence, and conclusions. Topics include prevalence of obesity in children, body composition, physiological changes, and pharmacokinetics dynamics.

E N D
Dosing considerations in obese children Dr Hussain Mulla
Should drug doses be adjusted for obese children? Hussain Mulla PhD MRPharmS Senior Research Pharmacist, Paediatric Clinical Pharmacology Centre for Therapeutic Evaluation of Drugs in Children
Workshop • Epidemiology / Definitions • Body composition & (Patho) Physiology of obese children • Pharmacokinetic Parameter Changes • Clinical Evidence • Conclusion
Defining Obesity in Children BMI is defined as the weight in kilograms divided by the square of the height in meters (kg/m2).
Defining Obesity in Children • Underweight: BMI below the 5th percentile • Normal weight: BMI at the 5th and less than the 85th percentile • Overweight: BMI at the 85th and below 95th percentiles • Obese: BMI at or above 95th percentile
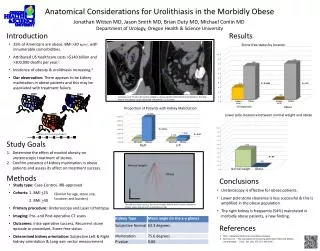
Body Composition of Obese Children • Obese children are taller (reflecting earlier maturation) and this needs to be taken into account when comparing proportion of fat and lean tissue • Obese children have • A larger absolute fat mass (FM) • A larger absolute lean body (fat free) mass (LBM) than non-obese children of the same age, gender and height.
Body Composition of Obese Children • As a rule of thumb 75% excess weight is fat – majority located in abdominal region but substantial also in the leg • The percentage of LBM calculated per kg of total bodyweight (TBW) is actually reduced • Obese children also have an increased hydration of lean mass, which has been attributed to an expanded extracellular water space. As LBM incorporates total body water, overhydration inflates LM values.
Physiological change in obesity • Blood flow per gram of fat is significantly reduced in morbidly obese individuals than moderately obese or lean individuals • Alterations in levels of plasma proteins (e.g. AAG) has been reported • Obese children show a fatty degeneration of the liver (NAFLD), increases in ALT and AST. • Obese children have increased kidney weight, renal blood flow and GFR.
Group work: How do these changes affect how obese children are dosed? • Dosing obese children by actual body weight assumes no structural or functional differences between obese and non-obese children • But increase in weight does not arise from the same proportions of FM and LM • Does the body composition and physiological changes affect Pharmacokinetics? • (Absorption) • Volume of Distribution • Clearance (metabolism and excretion) • How does obesity affect Pharmacodynamics?
The volume of distribution (Vd) of drugs may be altered in obese patients. increased adipose tissue mass increased organ mass lean body mass Particularly relevant for acute dosing (loading doses) Cheymol G. Clin Pharmacokinet. 2000; 39:215-231. Distribution can influence moderate / highly lipophilic drugs can affect hydrophilic drugs
Distribution – Example 1 • rocuronium (vd = 0.2 L/kg) is a hydrophillic drug • Should be dosed according to Ideal Body Weight (a correlate of LBM)
Distribution – Example 2 E.g. aminoglycosides (0.3L/kg) distribute primarily into the intravascular space and only moderately into the interstitial space. Aminoglycosides typically display a slightly larger volume of distribution (in liters) in obese patients than in lean patients Dosing aminoglycosides using ideal body weight in obesity may result in supratherapeutic serum concentrations
Distribution – Example 3 Need to exercise caution with since lipophillic drugs do not necessarily distribute extensively into adipose tissue in vivo. E.g. remifentanil (0.5 L/kg) Steady state V per kg of TBW is smaller in obese patients Recommended that IBW be used to determine dose
Clearance • Maintenance doses are based on plasma clearance of the drug. • Principal clearance organs liver/kidney constitute LBM • LBM increases in obese children and therefore clearance of drugs is higher in obese children • However, % LBM per kg of TBW is reduced i.e. CL of drugs does not increase proportionally to TBW in obese children • Problem; no bed side equation for LBM in children
Clearance Solid curve: LBW 2005Dashed curve: Clearance Total Body Weight (kg)
Metabolism Phase I reactions observed to be unchanged or increased in obesity(1). Clindamycin and metronidazole are metabolized via Phase I reactions and may be affected by obesity (2). Increase Phase II drug biotransformation reported (1). E.g. lorazepam and oxazepam are metabolized by conjugation (3). 1. Blouin RA, Warren GW. J Pharm Sci. 1999; 88:1-7. 2. Blouin RA; Chandler MHH. Applied pharmacokinetics: principles of therapeutic drug monitoring. In: Evans WE, Schentag JJ, Jusko WJ, ed. Applied Therapeutics. 3rd ed. Vancouver, BC: Applied Therapeutics Inc; 1992:11.3-11.20. 3. Westphal JF, Brogard JM. Clin Pharmacokinet. 1993; 24:46-58.
Renal Elimination creatinine clearance is increased in healthy obese subjects in proportion to the estimated fat free mass. conflicting data regarding renal clearance of specific drug have been reported. obese patients often have morbidities such as diabetes and hypertension that are known to impair renal function. Therefore overestimation or underestimation of clearance can occur in obesity.
Renal Elimination • Various equations commonly used to calculate glomerular filtration rate in children. • GFR (mL/min/1.73 m2) = k (Height) / Serum creatinine k = Constant k = 0.33 in preemie infants k = 0.45 in term infants to 1 year of age k = 0.55 in children to 13 years of age k = 0.70 in adolescent males (not females because of the presumed increase in male muscle mass, the constant remains .55 for females) Height in cm Serum creatinine in mg/dL • Their use is questionable due to the disparity between muscle mass and body weight ratio observed in obesity.
Renal Elimination The Salazar-Corcoran equation takes into account multiple factors to provide a better estimation of ClCr in obesity. (serum creatinine, gender, actual weight, age, and height). Complicated formula and not a particularly practical equation to use for quick reference.
Conclusion • There are no concrete recommendations • LD • Hydrophilic drugs, dose to IBW • Lipophillic drugs, may need to adjust dose to IBW/TBW. In the absence of clinical data, tread carefully (e.g. dose to TBW using a series of mini doses) • MD • Clearance predicted to increase with increasing LBM • Little supporting clinical data • In oncology concern expressed at methods employed to reduce doses in obese individuals • Consider dosing according to BSA (calculated using actual bodyweight)
Clearance Solid curve: LBW 2005Dashed curve: Clearance A more recent study presents a semi-mechanistic model for lean body weight (LBW)2005 that is sufficiently robust to quantify the influence of body composition on drug clearance, and could be therefore an ideal metric for adjusting chronic dosing in the obese. Solid curve: LBW 2005Dashed curve: old formula