Download
1 / 41
430 likes | 866 Views
“ Lymphocele ” After Kidney Transplantation. 2001.04.20 R4 이완수. Renal Replacement Therapy in ESRD Dialysis : Hemodialysis (HD) Peritoneal dialysis (PD) Kidney transplantation (KT). Benefits of KT : compared with dialysis Quality of life ↑ Long-term mortality ↓

E N D
“Lymphocele” After Kidney Transplantation 2001.04.20 R4 이완수
Renal Replacement Therapy in ESRD • Dialysis : Hemodialysis(HD) Peritoneal dialysis (PD) • Kidney transplantation (KT)
Benefits of KT : compared with dialysis • Quality of life ↑ • Long-term mortality ↓ • Patient survival ↑ • Cost effectiveness ↑ • The largest benefit : patients 20 to 39 ys of age, including diabetics
Monitoring for potential surgical & medical complications • Early diagnosis and appropriate intervention can minimize the detrimental impact on the graft & recipient
Medical Complication in KT • Rejection; Acute rejection Chronic allograft nephropathy(CAN) • Malignancy • Cardiovascular disease • Bone disorder • Infectious disease (CMV, BK virus, UTI, Hepatitis B&C …) • Recurrence of primary disease • Pregnancy 1) 초급성 거부반응 (Hyperacute rejection) : 이식 후 수분 또는 수시간 2) 가속성 급성 거부반응 (Accelerated acute rejection) : 이식 후 5~7일 이내 3) 초기 급성 거부반응 (Early acute rejection) : 이식 후 1주~12주 4) 후기 급성 거부반응 (Late acute rejection) : 이식 후 12주 이후 • HBV/HCV -- HCC • EBV -- PTLD(Post-transplantation lymphoproliferative disease) • HPV -- Squamous cell cancer • HHV-8 -- Kaposi’s sarcoma 면역억제제 코티코스테로이드, 칼시류린억제제(calcineurin inhibitors), 타크로리무스(tacrolimus) 이식 신 만성 동종이식 신병증(chronic allograft rejection) 이식 신 동맥 협착(graft artery stenosis) 원발성신질환 재발 또는 신생 사구체신염(recurrent or de-noveglomerulonephritis) 급, 만성 거부반응(acute and chronic rejection) 약제에 의한 독성(drug-induced nephropathy) 이식 신 요로폐쇄(graft outflow obstruction; lymphocele, ureteralstenosis) 원발 신에서의 고레닌 합성 다혈구증(polycythemia) 고칼슘혈증(hypercalcemia) 원발성 고혈압 또는 이차성 고혈압의 동반 • Hypercalcemia • Hypophosphatemia • Hyperparathyroidism • Osteoporosis • Fracture • Avascular necrosis • Post-transplant Bone Pain Syndrome Cadaver donor: 2년 후, Living donor: 1.5년 후 고려 Serum creatinine <2.0 ㎎/dL BP <140/90 mmHg 최근 6개월 동안 급성거부반응이 없을 것 PDS 하루 15 ㎎ 이하 투여 시 자궁내 성장 지연은 없다 면역억제제의 독성 발생이 가능하므로 수유는 금함
Surgical Complication in KT • Hemorrhage • Vascular complications • Urologic complications • GI complications • Lymphocele • Uncommon • Donor vessels • Renal artery thrombosis • Renal artery stenosis • Renal vein thrombosis • Recipient vessels • Iliac artery thrombosis • Iliac artery pseudoaneurysms • Deep venous thrombosis • Pulmonary embolism • Urinary tract obstruction • Blood clot in the bladder or urethral catheter • Obstruction of ureteroneocystostomy • Ureteral obstruction • Urinary leakage
INTRODUCTION • Lymphocele • lymphatic collection around a transplanted kidney • Diagnosis • pelvic collection with similar properties to the plasma • biochemical analysis of the fluid similar electrolyte low protein level • On microscopic evaluation • presence of lymphocytes can be a useful clue.
INTRODUCTION • Biochemical analysis of lymphocele • 혈청치와 거의 같은 것 • BUN, Creatinine • Na, K, Cl • CO2, P, Bilirubin, Uric acid, Glucose, AST • 혈청치보다 낮은 것 • Cholesterol, Ca, LDH, SAP • Protein • Albumin, α1 globulin, α2globulim, βglobulim, IgG, IgA, beta1C • 혈청치보다 높은 것 • Aldolase, Acid phosphatase
INTRODUCTION • Occurrence • 2 wks ~ 6 months after KT • peak incidence : 6 wks • delayed formation : 8 yrs after KT • Incidence • 12% to 40% of transplant recipients • clinically significant lymphocele “20%”
INTRODUCTION • Ultrasonography • 1/2 of transplanted kidneys, collections (≤ 50 cm3) can be detected • most of which are ≤ 3 cm in diameter resolve spontaneously • most of the lymphatic collections are Subclinical
ETIOLOGY • DiessectedVessel? • 곧 수축하는 성질 • But, Lymphatic duct? • clotting factor (-) • 잘린후,48시간 까지는 폐쇄되지 않음 • High frequency in KT? WHY? • KT pt. ? • 다량의 steroid 사용과 그전의 uremia 때문에 지연됨 CF) Lymphatic duct regeneration • 정상적인 경우 7~10일만에 재생 • Low-steroid regimens for immunosuppression?? • lymphocelehas decreased?? Controversial
ETIOLOGY • Radioisotope studies • suggest that most lymphoceles • originate from • Leakage of lymph from unligated iliac vessel lymphatics of the recipient Drainage route of the lower limb lymphatic vessels is along the iliac vessels. ( when the iliac vessels are mobilized for anastomosis some lymphatic vessels are unavoidably divided) 2. Lymphocele can also originate from transplanted kidney lymphatic vessels.
ETIOLOGY • In a study by Sansalone and colleagues • cephalad implantation of the kidney in the ipsilateral iliac fossa to the common iliac vessels (less lymphatic manipulation) • in comparison with standard operation (in the contralateral iliac fossa and anastomosis to the external iliac vessels) • significant lower rate of lymphocele formation(2.1% vs 8.5%)
ETIOLOGY • Hamza and colleagues • No relationship between • the extent of iliac vessel preparation and lymphocele occurrence • however, to prevent lymphocele formation • transplanted bed be restricted to the least possible • lymphatic vessels be ligated precisely at the hilumof the kidney allograft. • all of lymphatic vessels must be tied or clipped, but diathermy is not suggested.
ETIOLOGY Drainage route of the lower limb lymphatic vessels is along the iliac vessels. (when the iliac vessels are mobilized for anastomosis some lymphatic vessels are unavoidably divided) 2. Lymphocele can also originate from transplanted kidney lymphatic vessels. • Why?? Unexplained • Probably, the inflammatory process associated with allograft presence increases the flow of lymph from lymphatic vessels around the iliac vessels.
ETIOLOGY • Immunosuppressive regimens • In a study by Goel and colleagues • combination of sirolimus, mycophenolatemofetil, and prednisone • independent factor for lymphocele occurrence - mechanism? • delayed healing of wound and injured lymphatic vessels. • Langer and Kahan • impact of sirolimus risk of lymphocele ↑ • Tondolo and colleagues questioned this mechanism!! • incidence of lymphocele is similar in multiple immunosuppressive regimens
ETIOLOGY • Obestiy • longer operative time • more frequently suffer from wound infection, perinephric hematoma, and lymphocele. ★ obesity (BMI 30 kg/m2↑) independent risk factor for lymphocele formation
ETIOLOGY • High molecular weight heparin (HMWH) • graft losses ↓ secondary to thrombosis or vascular rejection • But, incidence of lymphocele↑ • Lundin and colleagues • 130 kidney allograft recipients • frequency ↑of lymphocele with heparin prophylaxis • 43% vs 20%
ETIOLOGY • Rejection episodes • may have a role in lymphocele formation • In a study by Lipay and colleagues • high frequency of cellular rejection in patients with lymphocele was indicative of a possible cause-effect relationship • In another study on 115 patients • multivariate analysis of possible lymphocele risk factors • only rejection was accompanied by high risk of lymphocele formation • allograft rejection was most important contributing factor in lymphocele formation
CLINICAL MANIFESTATIONS • clinically silent (most) • other presentations • Hypertension • Pain • Fever • Frequency • ipsilateralthrombophlebitis • palpable mass • lymphatic fistula. • urinary retention due to compressive effect • common manifestation • impaired graft function • perigraft collection • unilateral leg edema
DIAGNOSIS • Ultrasonography • Key to diagnosis of lymphocele • Homogeneity, specific shape and position • inferior to the lower pole of the transplanted kidney (most) • obviously separate from the bladder • Infective lymphoceles • complex echo pattern inside the kidney • Repeated ultrasonography after bladder drainage • can differentiate the presence of lymphocele from a full bladder
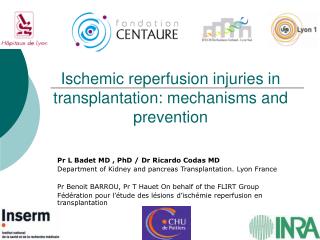
Lymphocele, Longitudinal US image demonstrates a large hypoechoic fluid collection adjacent to the renal transplant (arrow).
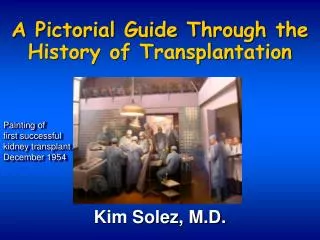
Lymphocele, Transverse US image of the midpole region of a renal transplant shows a large anechoic fluid collection adjacent to the renal hilum
Lymphocele, (b) Longitudinal color Doppler image shows hydronephrosis resulting from extrinsic compression of the collecting system.
DIAGNOSIS • Dynamic renal scintigraphy(Technetium Tc-99m diethylenetriaminepentaacetic acid) For routinely followed up • Kumar and colleagues, 3 patterns for lymphoceles were described: • 1. an initial photopenic area that progressively fills with tracer activity with an equal level to the background activity in delayed films • 2. initial photopenic areas with an activity more than the background activity in delayed films • 3. persistent photopenic areas in early and delayed films. • Rim of increased activity of tracer around the initial photopenic area in some patients in favor of lymphocele diagnosis
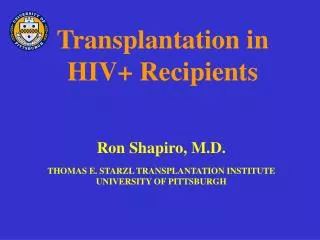
(a) (b) Lymphocele. (a) Views from a Tc-99m MAG3 study demonstrate the appearance of the normal transplant in the right lower quadrant. (b) Views from a repeat study performed 2 months later show that the upper pole of the transplant is compressed by a large photopenic defect (arrows).
DIAGNOSIS • Intravenous Urography • Computed Tomography • not necessary in typical cases • only in complicated or equivocal ones
Differential diagnosis • 1. Acute rejection • Lymphocele과 acute rejection이 동반되는 경우가 많음 • 단순히 rejection이라고 생각하고 steroid 등을 다량으로 사용시 lymphocele악화 • 2. Thrombophlebitis • Lymphocele에 의해 IVC, iliac vein compression으로 발생 • PTE 발생 가능 • 3. Acute pyelonephritis • Lymphocele에 의해 비뇨관계 폐색으로 발생 가능 • 4. Pseudocyst • Hematoma, urinoma, abscess와 외형으로 구별 힘듬
MANAGEMENT • Conservative Management • Small asymptomatic collections are common • usually resolve spontaneously • conservative management can be satisfactory
MANAGEMENT • Simple Aspiration • Ultrasonography-guided aspiration • not only diagnostic, but also therapeutic in selected cases • initial treatment modality • relief of urinary obstruction • recovery of kidney function • prevention of emergency situation • Sometimes, multiple sessions of aspiration is necessary • Rate of spontaneous recovery reduces after 3 recurrences • each aspiration brings about a low risk of infection
Percutaneous drainage of a lymphocele. Longitudinal US image obtained during needle placement shows the echogenic needle within the fluid collection (arrow).
Sclerotherapy • external drainage via percutaneous catheter • administration of a sclerosing agent (instillation) • Ethanol • Povidone iodine • Tetracycline • Recurrences (20%↑)
Surgery • intraperitoneal drainage of lymphocele • local symptoms, graft dysfunction 있을때 first line of the treatment • effectiveness ↑ • safety ↑ • named incorrectly as “marsupialization” • “unroofing “or “fenestration” is more precise
Surgery . • Laparoscopy • effective minimally invasive treatment • excellent alternative for open surgery • “Transplanted ureter”, “bladder” injury – possible • Bulging induced by extraperitoneal kidney sometimes mistaken by lymphocele • “intra-operative ultrasonography” avoid organ injury during laparoscopy • Recurrence rate : 5 ~ 13%
Surgery • Open surgery • required in patients with a previous abdominal surgery • lymphoceles with inappropriate characteristics or location • other simultaneous procedures should be done • deep lymphoceles around the lower pole of the kidney (open surgery is safer) • thick wall of lymphocele • bladder rupture during laparoscopy
COMPLICATIONS • Most lymphocelesare managed without complication • But, infections in an immunocompromised recipient may be a problem (especially with organisms like yeasts) • impaired graft function • pressure effect on the renal vein or iliac veins venous thrombosis
Summary • Etiology • Extensive mobilization of the iliac vessels • Failure to ligate the lymphatics crossing • Incidence: 0.6 - 18% • Symptoms • Swelling of the wound • Edema of the scrotum, labia, and lower extremity • Urinary obstruction from pressure • Diagnosis • Ultrasound : Perinephric fluid collection • Treatment • Aspiration : Temporary benefit • Percutaneous drainage • Fenestration of the cyst into the peritoneal cavity Definitive surgery, often laparoscopically
Monitoring for potential surgical & medical complications • Early diagnosis and appropriate intervention can minimize the detrimental impact on the graft & recipient