Download
1 / 12
140 likes | 392 Views
Overcoming Impenetrable Barrier to Transplantation: ABO Blood Group Incompatibility. Reference: Joseph Kahwaji J, Vo AA, Jordan SC. ABO blood group incompatibility: A diminishing barrier to successful kidney transplantation? Expert Rev Clin Immunol . 2010;6(6):893–900.

E N D
Overcoming Impenetrable Barrier to Transplantation: ABO Blood Group Incompatibility Reference: Joseph Kahwaji J, Vo AA, Jordan SC. ABO blood group incompatibility: A diminishing barrier to successful kidney transplantation? Expert Rev ClinImmunol. 2010;6(6):893–900.
ABO Blood Group Incompatibility: A Note • The last 30 years saw the significant improvements in the outcomes in kidney transplantation with the development of maintenance and induction immunosuppression and antimicrobial prophylaxis. • Particularly the last decade witnessed the emergence of new antibody reduction and immunomodulatory therapies that played a larger role in the development of desensitization techniques to modulate anti-HLA or antiblood group antibodies, thus making incompatible transplantation possible. • Above all, the combination of antibody reduction using plasma exchange (PE), intravenous immunoglobulin (IVIg; antibody reduction and immunomodulation) and B-cell depletion using rituximab have shown impressive benefits in removing the immunologic barriers to successful transplantation. • Over the last decade, blood type-incompatible transplantation has gained wide acceptance.
Role of B1 Cells • A distinct type of B cell (B1) that exists in the marginal zones of the spleen and peritoneum, produce ‘natural antibodies’, primarily of the IgMisotype, but also IgG and IgAisotypes. • These antibodies are produced in the absence of external antigenic stimulation and have a stable but broad reactivity pattern. • Moreover, they recognize a number of self-antigens, altered self, carbohydrate sequences, phospholipids, amyloid b-peptide and surface glycoproteins. • These cells are self-regenerating and possibly represent a ‘hard-wired’ immune response aimed at invading pathogens, altered self and blood group antigens; besides possessing extensive cross-reactivity. • Consequently, B1 cell responses are independent of T cells and are probably more susceptible to modification by B-cell-directed therapies.
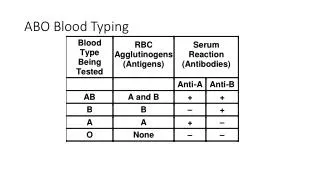
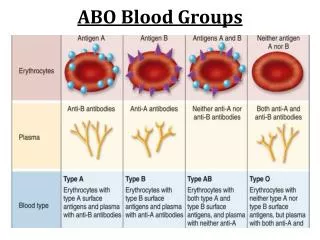
Immunologic Hurdles to ABOi Transplantation • The existence of natural antibodies against blood group antigens is the root for the acute antibody-mediated rejection (AMR) and accelerated graft failure seen in early experience with ABOi. • Red blood cells express carbohydrate structures on their cell surfaces, designated A and B, that cause agglutination when bound by antibody. • These antigens are also expressed on other tissues, including renal endothelium. • Antibodies, classified as IgG and IgM, acting against these blood groups develop naturally as bacteria present in the gut express similar antigens. • As a result, blood type-incompatible transplantation cannot take place without removing or modulating the natural antibody response to blood group antigens.
Immunologic Hurdles to ABOi Transplantation • The difficulty of ABOi was originally documented in the 1950s and 1960s. • Recipients of a blood typeincompatible allograft developed severe AMR and graft loss after transplantation. • Fortunately after 1999, graft survival improved significantly with the use of tacrolimus and mycophenolate mofetil as part of the induction and maintenance immunosuppression with splenectomy. • Subsequently, ABOi transplantation was at an impasse until the concept of a ‘medical splenectomy’ was discovered in patients treated with rituximab (anti-CD20, anti-B cell).
Role of Rituximab in B-cell Depletion • Originally approved in 1997, rituximab was used for the treatment of non-Hodgkin’s lymphomas and, shortly afterward, for rheumatoid arthritis. • Since then, it has shown good outcomes in various autoimmune and inflammatory diseases. • In kidney transplantation, it is found effective for the treatment of post-transplant lymphoproliferative disorder, AMR, desensitization and recurrent or de novo glomerulonephritis in the renal allograft. • Rituximab targets against the CD20 antigen located on mature and some premature B cells. • The antibody binds to its target and eliminates B cells via complementdependentcytotoxicity, antibody-dependent cell-mediated cytotoxicity and apoptosis. • This effectively depletes B cells in the peripheral blood, lymph nodes and the spleen. • Additionally, rituximab has an effect on memory B cells, revealing a delay in the recovery of memory B cells. • This effect could be responsible for preventing a memory response after transplantation and differentiation of B cells to plasma cells.
The Modern Era Use of Rituximab in ABOi • Splenectomy is at present rarely used in ABOi transplantation and is probably not compulsory. • Studies have shown that administration of rituximab without splenectomy was sufficient for successful transplantation. • On top, only one dose of rituximab was needed to achieve these outcomes. • The prevention of antibody rebound by rituximab combined with antibody removal emerges as sufficient to safely proceed with ABOi transplantation without splenectomy. • Short-term results have been good when using a single dose of rituximab in combination with antibody removal and immunosuppression.
Even long-term outcomes support the efficacy of regimens that utilize rituximab in ABOi. • Recently, factors that influence poor graft survival in ABOi transplantation have been identified. • There was a drastically worse graft survival in those that had donor-specific antibody present at the time of transplantation, and did not receive mycophenolate mofetil prior to transplant or did not achieve a titer of less than 1:32 at the time of transplantation. • Long-term outcomes with rituximab have been similar to ABOcompatible living-donor transplantation when these criteria have been met. • Long-term outcomes in those that receive an ABO-compatible transplant, ABOi transplant with splenectomy and ABOi transplant with rituximab (no splenectomy) have also been reported, revealing that the patient and graft survival and renal function were similar at 3 years among all the groups. • Interestingly, there was an increase in the risk of AMR in the ABO-compatible and splenectomy group compared with the group that received rituximab.
Is Rituximab Necessary in ABOi Transplantation? • Rituximab is a critical component of ABOi transplantation. • The protocol at Cedars-Sinai (Los Angeles, CA, USA) consists of administering mycophenolate mofetil 1 month prior to transplant, and 1 g rituximab 2 weeks prior to transplant. • This is followed by five sessions of plasmapheresis with IVIg (2 g/kg, max 140 g) after the final PE session (see Fig. 1).
The good outcomes confirmed that rituximab appears to limit antibody rebound after transplantation and may also have long-term immunomodulatory effects on Tcell- mediated effector functions. • A decrease in anti-A/B antibodies, particularly IgM, has been noted after rituximab administration. • Besides, rituximab has shown to decrease the anti-HLA antibodies in a group of patients with chronic kidney disease on dialysis. • This limits the need for posttransplantplasmapheresis, which can be costly and increase bleeding and infectious complications. • It has also been found the administration of rituximab to be safe with a low rate of infectious complications. • Current data suggest that the inclusion of rituximab in ABOi preconditioning is important.
Summary • The introduction of rituximab has dramatically shaped the development of ABOi transplantation globally. • Splenectomy is no longer required, making ABOi more pleasant to physicians and patients alike. • With the appropriate laboratory, clinical and renal pathology teams organized and dedicated to ABOi transplantation, it can now be performed at any transplant center. • The ‘three pillars’ of ABOi transplantation include PE, IVIg and B-cell depletion with rituximab. • Implementing the ABOi protocols will have a substantial impact on increasing the number of kidney transplants performed worldwide, besides improving the length and quality of life for several patients.