Download
1 / 35
440 likes | 529 Views
Focus on Tube Feeding. (Relates to Chapter 40, “Nursing Management: Nutritional Problems,” in the textbook). Oral Feeding. High-calorie supplements Used when nutritional intake is deficient Examples include Milkshakes Puddings Ensure, Sustacal Used as snacks. Tube Feeding.

E N D
Focus on Tube Feeding (Relates to Chapter 40, “Nursing Management: Nutritional Problems,” in the textbook)
Oral Feeding • High-calorie supplements • Used when nutritional intake is deficient • Examples include • Milkshakes • Puddings • Ensure, Sustacal • Used as snacks
Tube Feeding • Also known as enteral nutrition • Administration of nutritionally balanced liquefied food or formula through tube inserted into • Stomach • Duodenum • Jejunum
Tube Feeding (Cont’d) • Provide nutrients to GI tract alone or supplemental to oral or parenteral nutrition • Easily administered • Safer than parenteral • More physiologically efficient than parenteral • Less expensive than parenteral
Tube Feeding (Cont’d) • Indications include those with • Anorexia • Orofacial fractures • Head/neck cancer • Burns • Nutritional deficiencies
Tube Feeding (Cont’d) • Indications include those with • Neurologic conditions • Psychiatric conditions • Chemotherapy • Radiation therapy
Tube Feeding (Cont’d) • Delivery options include • Continuous infusion by pump • Intermittent by gravity • Intermittent bolus by syringe • Cyclic feedings by infusion pump
Tube Feeding • Nasogastric and nasointestinal tubes • Inserted through the nasal cavity • Radiopaque: Allowing visualization from X-ray • ↓ Likelihood of regurgitation and aspiration when placed in intestine
Tube Feeding (Cont’d) • Nasogastric and nasointestinal tubes • Can be dislodged by vomiting or coughing • Can be knotted/kinked in GI tract
Tube Feeding (Cont’d) • Gastrostomy and jejunostomy tubes • May be used in those needing tube feedings for extended period • Patient must have intact, unobstructed GI tract • Can be placed surgically, radiologically, or endoscopically
Placement of Gastrostomy Tube Fig. 40-5
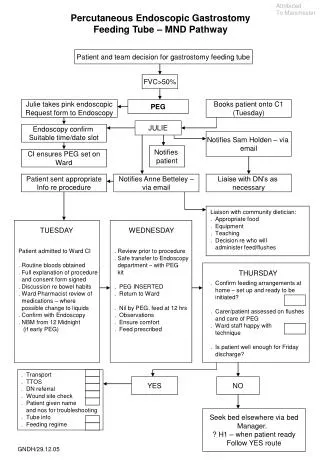
Tube Feeding • Percutaneous endoscopic gastrostomy (PEG) placement requires esophageal lumen wide enough for endoscope • PEG and radiologically placed gastrostomy • Fewer risks than surgical placement, lower cost, minimum sedation
Percutaneous EndoscopicGastrostomy • Gastrostomy tube placement via percutaneous endoscopy • Using endoscopy, a gastrostomy tube is inserted through esophagus into stomach and then pulled through a stab wound made in abdominal wall Fig. 40-6 A
Percutaneous Endoscopic Gastrostomy (Cont’d) • Retention disk and bumper secure the tube Fig. 40-6 B
Tube Feeding • Feedings can be started when bowel sounds are present, usually 24 hours after placement • Immediately after insertion, tube length from insertion site to distal end should be measured and recorded
Tube Feeding (Cont’d) • Tube should be marked at skin insertion site • Insertion length should be checked regularly
Tube Feeding (Cont’d) • Tube feeding administration • Patient position • Patient should be sitting or lying with HOB at 30 to 45 degrees • HOB remains elevated for 30 to 60 minutes for intermittent delivery
Tube Feeding (Cont’d) • Tube feeding administration • Tube patency • Irrigated with water before/after each feeding, drug administration, residual checks • Continuous feedings administered on feeding pump with occlusion alarm
Tube Feeding (Cont’d) • Tube position • Placement checked before each feeding/drug administration or every 8 hours with continuous feeds
Tube Feeding (Cont’d) • Tube position (cont’d) • Methods used to check placement • Aspiration of stomach contents • pH check • pH less than 5: Indicative of stomach • Most accurate assessment: X-ray visualization
Tube Feeding (Cont’d) • Tube position (cont’d) • Check gastric residual volumes • ↑ Volume leads to aspiration
Tube Feeding (Cont’d) • Formula • Before feeding • Aspirate gastric contents and measure amount • Volume greater than 150 ml and clinical signs of intolerance—feeding held for 1 hour and residual rechecked • More than 110% of hourly rate of pump—hold feeding • Residual should be given back to patient
Tube Feeding (Cont’d) • Formula • Commercial formulas are preferred to blenderized foods • Room/body temperature
Tube Feeding (Cont’d) • Administration of feedings • Pump • Gradually increase rate or volume over 24 to 48 hours • Intermittent feedings • Volume usually 200 to 500 ml per feeding • Administer flush water or water boluses as tolerated
Tube Feeding (Cont’d) • General nursing considerations • Daily weights • Assess for bowel sounds before feedings • Accurate I&O • Initial glucose checks • Label with date and time started • Feedings infusing >8 hours discarded • Pump tubing changed q24h
Tube Feeding (Cont’d) • Complications • Vomiting • Diarrhea • Constipation • Dehydration • More calorically dense, less water formula contains • Check for high protein content
Tube Feeding (Cont’d) • Gastrostromy or jejunostomy feedings • Two potential problems • Skin irritation • Skin assessment and care • Pulling out of tube • Education to patient/family regarding feeding administration, tube care, and complications
Tube Feeding • Gerontologic Considerations • More vulnerable to complications • Fluid and electrolyte imbalances • Glucose intolerance • Decreased ability to handle large volumes • Increased risk of aspiration
Case Study • 84-year-old male is being discharged from the hospital • He was admitted with complications from esophageal cancer
Case Study (Cont’d) • PEG tube has been placed to allow for tube feedings • He lives with his wife, who is 82-years-old • Has no other family in town
Discussion Questions • What risks are associated with a PEG that you should discuss with him and his wife? • What skills must he and his wife learn before discharge?
Discussion Questions (Cont’d) • Should any additional patient teaching be done before discharge? • How should his response to treatment be managed?