Download

1 / 55
550 likes | 920 Views
DR. IMTIAZ AHMED TAGO MBBS,FCPS ( ORTHOPEDIC SURGERY ) ASSISTANT PROFFESSOR DOST UNIT II LUMHS JAMSHORO. OSTEOARTHRITIS OSTEOARTHROSIS DEGENERATIVE JOINT DISEASE. DEFINITION. Osteoarthritis OA is a degenerative disease of diarthrodial ( synovial ) joints , characterized by

E N D
DR. IMTIAZ AHMED TAGOMBBS,FCPS (ORTHOPEDIC SURGERY)ASSISTANT PROFFESSORDOST UNIT II LUMHS JAMSHORO
DEFINITION • Osteoarthritis OA is a degenerative disease of diarthrodial (synovial) joints, characterized by • Breakdown of articular cartilage • and proliferative changes of surrounding bones
EPIDEMIOLOGY • Osteoarthritis(OA) is the most common joint disease • OA of the knee joint is found in 70% of the population over 60 years of age • Radiological evidence of OA can be found in over 90 % of the population
LIMITED FUNCTION • OA may cause functional loss • Activites of daily living • Most important cause of disability in old age • Major indication for joint replacement surgery
CHARACTERISTICS OF OA • OA is a chronic disease of the musculoskeletal system,without systemic involvement • OA is mainly a noninflammatory disease of synovial joints • No joint ankylosis is observed in the course of the disease
CLASSIFICATION OF OA • Primary OA Secondary OA Etiology is unknown Etiology is known
AGE • Primary OA > 40 years • Direct correlation • Aging process
RISK FACTORS FOR PRIMARY OA • Age • Sex • Obesity • Genetics • Trauma (daily)
SECONDARY OSTOARTHRITIS • Trauma • Previous joint disorders; • Congenital hip dislocation • Infection: Septic arthritis, Brucella, Tb • Inflammatory: RA, AS • Metabolic: Gout • Hematologic: Hemophilia • Endocrine: DM
ETIOLOGY OF OA • Cartilage properties • Biomechanical problem
STRUCTURE OF JOINT CARTILAGE • Collagen (Type 2) • Proteoglycan - Hyaluronic acid - Glycoseaminoglycan • Water • Condrocyte Regeneration and Degeneration
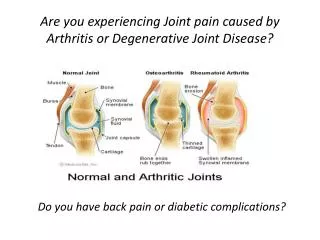
PATHOLOGY OF OA • Fibrillation • Eburnation • Osteophytes • Subcondral cysts
LABORATORY FINDINGS OF OA • There are no pathognomonic laboratory findings for OA • Laboratory analysis is performed for differential diagnosis
RADIOLOGIC FINDINGS OF OA • Narrowing of joint space (due to loss of cartilage) • Osteophytes • Subchondral (paraarticular) sclerosis • Bone cysts
RADIOLOGIC GRADE OF OA • G1 Normal • G2 Mild • G3 Moderate • G4 Severe • Kellgren Lawrence Classification
DIAGNOSIS OF OA CLINICAL FINDINGS Joint pain + RADIOLOGIC FINDINGS Osteophytes
CLINIC OF OA SIGNS AND SYMPTOMS • Joint pain - degenerative • Stiffness following inactivity – 30 min • Limitation of ROM – later stages • Deformity – restricition of ADL
OA OF KNEE JOINT (GONARTHROSIS) • More common in obese females • over 50 years of age • Joint stiffness (<30 minutes) • Mechanical pain • Physical examination findings: Crepitus • Pain on pressure • Painful ROM and functional limitation • Limitation of ROM in later stages of OA (first extension) • Laboratory analysis within normal limits
OA OF HIP JOINT • More common in males over 40 years of age • Joint stiffness • Pain of hip,gluteal and groin areas radiating to the knee (Nobturatorius) • Mechanical pain • Limited walking function
COXARTHROSIS Physical examination: • Antalgic limping • Limitation of ROM (first internal rotation) • Painful ROM • Trendelenburg test positivity • Leg length discrepancy Laboratory analysis within normal limits
Peripheral Joints • Hands • Feet
ETIOPATHOGENESIS OF OA • Age,gender Local • Genetic OA biochemical effects • Other factors
ETIOPATHOGENESIS OF OA • Dysfunction of joint cartilage • Condrocyte function:1- Degredative enzymes (metalloproteases) 2- Inhibitors Degeneration and regeneration functions are balanced • IL-1 , degredative enzymes + synovial inflammation results:Breakdown of cartilage
PATHOGENESIS OF OA • Cytokines IL-1, IL-6, TNF- • Cell destruction • Membrane phospholipids • Arachidonic acid • Cox-1, Cox-2
IL-1 and metalloproteases have been found to play an important role in cartilage destruction. • Local growth factors,especially transforming growth factor (TGF) are involved in the formation of osteophytes
TREATMENT OF OA • Symptomatic treatment • Structure modifying treatment • Surgical treatment
STRUCTURE MODIFYING TREATMENT • Hyaluronic acid injection (HA) • Glycose amino glycans (GAG)
PRIMARY PREVENTION OF OA ?? • Regular exercises • Weight control • Prevention of trauma
AIMS OF OA TREATMENT • Pain relief • Preservation and restoration of joint function • Education
Non-Pharmacologic Treatment of OA • Patient education • Weight loss (if overweight) • Aerobic exercise programs • Physical therapy • Range-of-motion exercises Muscle-strengthening exercises • Assistive devices for ambulationPatellar tapingAppropriate footwear Lateral-wedged insoles (for genu varum) • Bracing • Occupational therapy • Joint protection and energy conservation
PHARMACOLOGIC TREATMENT OF OA • Oral Systemic Medical Agents - Analgesics (acetaminophen) - NSAIDs - Opioid analgesics • Intraarticular agents: Hyaluronan Glucocorticoids (effusion) • Topical agents