Download

1 / 48
510 likes | 576 Views
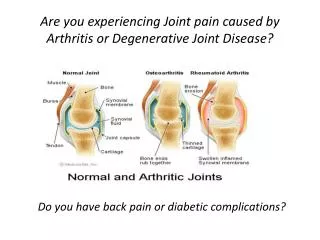
OSTEOARTHRITIS DEGENERATIVE JOINT DISEASE. DEFINITION. Osteoarthritis OA is a degenerative joints disease, characterized by B reakdown of articular cartilage and proliferative changes of surrounding bones. Synovial inflammation

E N D
DEFINITION • Osteoarthritis OA is a degenerative joints disease, characterized by • Breakdown of articular cartilage and proliferative changes of surrounding bones. • Synovial inflammation • OA is a chronic disease of the musculoskeletal system,without systemic involvement
EPIDEMIOLOGY • Osteoarthritis(OA) is the most common joint disease • OA of the knee joint is found in 70% of the population over 60 years of age • Radiological evidence of OA can be found in over 90 % of the population
LIMITED FUNCTION • OA may cause functional loss • Activites of daily living (ADL) • Most important cause of disability in old age • Major indication for joint replacement surgery
CLASSIFICATION OF OA • Primary OA Secondary OA Etiology is unknown Etiology is known
AGE • Primary OA > 40 years • Direct correlation • Aging process
RISK FACTORS FOR PRIMARY OA • Age • Sex • Obesity • Genetics • Trauma (daily)
SECONDARY OSTOARTHRITIS • Trauma • Previous joint disorders; • Congenital hip dislocation • Infection: Septic arthritis, Brucella, Tb • Inflammatory: RA • Metabolic: Gout • Hematologic: Hemophilia • Endocrine: DM
ETIOLOGY OF OA • Cartilage properties • Biomechanical problem
Pain is related to use Pain gets worse during the day Minimal morning stiffness (<20 min) and after inactivity (gelling) Range of motion decreases Joint instability Bony enlargement Deformity – restricition of ADL Restricted movement Crepitus Variable swelling and/or instability OA: Symptoms and Signs
LABORATORY FINDINGS OF OA • There are no pathognomonic laboratory findings for OA • Laboratory analysis is performed for differential diagnosis
RADIOLOGIC FINDINGS OF OA • Narrowing of joint space (due to loss of cartilage) • Osteophytes • Subchondral (paraarticular) sclerosis • Bone cysts
RADIOLOGIC GRADE OF OA • G1 Normal • G2 Mild • G3 Moderate • G4 Severe • Kellgren Lawrence Classification
DIAGNOSIS OF OA CLINICAL FINDINGS Joint pain + RADIOLOGIC FINDINGS Osteophytes
OA OF KNEE JOINT • More common in obese females • over 50 years of age • Joint stiffness (<30 minutes) • Mechanical pain • Physical examination findings: Crepitus • Pain on pressure • Painful ROM and functional limitation • Limitation of ROM in later stages of OA (first extension) • Laboratory analysis within normal limits
OA OF HIP JOINT • More common in males over 40 years of age • Joint stiffness • Pain of hip,gluteal and groin areas radiating to the knee • Mechanical pain • Limited walking function
Hip Osteoarthritis Physical examination: • Antalgic limping • Limitation of ROM • Painful ROM • Leg length discrepancy Laboratory analysis within normal limits
Peripheral Joints • Hands • Feet
STRUCTURE OF JOINT CARTILAGE • Collagen (Type 2) • Proteoglycan - Hyaluronic acid - Glycoseaminoglycan • Water • Condrocyte Regeneration and Degeneration
ETIOPATHOGENESIS OF OA • Age,gender Local • Genetic OA biochemical effects • Other factors
ETIOPATHOGENESIS OF OA • Dysfunction of joint cartilage • Condrocyte function:1- Degredative enzymes (metalloproteases) 2- Inhibitors Degeneration and regeneration functions are balanced • IL-1 , degredative enzymes + synovial inflammation results:Breakdown of cartilage
PATHOGENESIS OF OA • Cytokines IL-1, IL-6, TNF- • Cell destruction • Membrane phospholipids • Arachidonic acid • Cox-1, Cox-2
IL-1 and metalloproteases have been found to play an important role in cartilage destruction. • Local growth factors,especially transforming growth factor (TGF) are involved in the formation of osteophytes
TREATMENT OF OA • Symptomatic treatment • Structure modifying treatment • Surgical treatment
PRIMARY PREVENTION OF OA ?? • Regular exercises • Weight control • Prevention of trauma
AIMS OF OA TREATMENT • Pain relief • Preservation and restoration of joint function • Education
Non-Pharmacologic Treatment of OA • Patient education • Weight loss (if overweight) • Aerobic exercise programs • Physical therapy • Range-of-motion exercises Muscle-strengthening exercises • Assistive devices for ambulationAppropriate footwear Lateral-wedged insoles • Bracing • Occupational therapy • Joint protection and energy conservation
Pharmacologic Management of OA • Non-opioid analgesics • Topical agents • Intra-articular agents • Opioid analgesics • NSAIDs • Unconventional therapies
Non-opioid Analgesic Therapy • First-line—Acetaminophen • Pain relief comparable to NSAIDs, less toxicity • Beware of toxicity from use of multiple acetaminophen-containing products • Maximum safe dose = 4 grams/day
Non-opioid Analgesic Therapy (cont’d) • NSAIDs • Use generic NSAIDs first • If no response to one may respond to another • Lower doses may be effective • Do not retard disease progression • Gastroprotection increases expense • Side effects: GI, renal, worsening CHF, edema • Antiplatelet effects may be hazardous
Non-opioid Analgesics in OA • Cyclooxygenase-2 (COX-2) inhibitors • Pain relief equivalent to older NSAIDs • Probably less GI toxicity • Side effects: Renal, edema • Older populations with multiple CV medical problems should be tested • Cost similar to generic NSAIDs plus proton pump inhibitor or misoprostol
Opioid Analgesics in OA • Tramadol • Affects opioid and serotonin pathways • Nonulcerogenic • May be added to NSAIDs, acetaminophen • Side effects: Nausea, vomiting, lowered seizure threshold, rash, constipation, drowsiness, dizziness
Opioid Analgesics for OA • Codeine, oxycodone • Long-acting oxycodone may have fewer CNS side effects • Propoxyphene • Morphine and fentanyl patches for severe pain interfering with daily activity and sleep
Topical Agents for Analgesia in OA • Local cold or heat: Hot packs, hydrotherapy • Capsaicin-containing topicals • Use well supported by evidence • Use daily for up to 2 weeks before benefit • Compliance poor without full instruction • Avoid contact with eyes • Liniments = methyl salicylates • Temporary benefit
Intra-articular steroids Good pain relief Most often used in knees, up to q 3 months With frequent injections; risk infection, worsening diabetes, or CHF Joint lavage Significant symptomatic benefit demonstrated Hyaluronate injections Symptomatic relief Improved function Require series of injections No evidence of long- term benefit Limited to knees Expensive OA: Intra-articular Therapy
OA: Unconventional Therapies • Polysulfated glycosaminoglycans—nutriceuticals • Glucosamine +/- chondroitin sulfate: Symptomatic benefit, no known side effects, long-term controlled trials pending • Tetracyclines as protease/cytokine inhibitors • Under study • Have disease-modifying potential
Surgical Therapy for OA • Arthroscopy • May reveal unsuspected focal abnormalities • Results in tidal lavage • Expensive, complications possible • Osteotomy: May delay need for TKR for 2 to 3 years • Total joint replacement: When pain severe and function significantly limited
OA: Management Summary • First: Be sure the pain is joint related (not a tendonitis or bursitis adjacent to joint) • Initial treatment • Muscle strengthening exercises and reconditioning walking program • Weight loss • Acetaminophen first • Local heat/cold and topical agents
OA: Management Summary (cont’d) • Second-line approach • NSAIDs if acetaminophen fails • Intra-articular agents or lavage • Opioids • Third-line • Arthroscopy • Osteotomy • Total joint replacement