Download
1 / 36
360 likes | 757 Views
Genitourinary Cancers. Janabel Said ST4 Clinical Oncology Ninewells Hospital. Topics. Renal Cancer Bladder Cancer Prostate Cancer Testicular Cancer Penile Cancer. Renal Cancer. 3% of all adult malignancies 30% presenting with metastatic disease M>F, ratio 5:3 50 – 80 years.

E N D
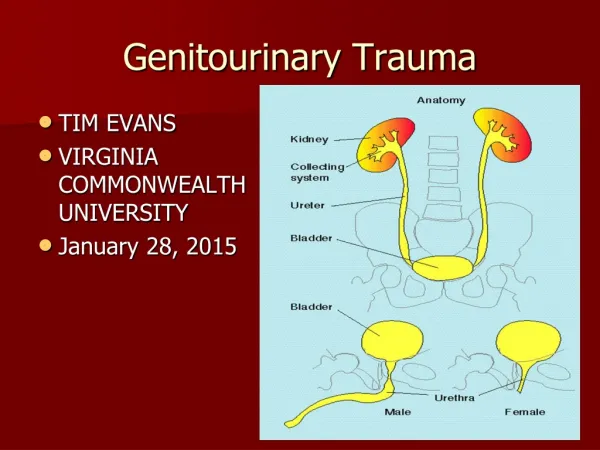
Genitourinary Cancers Janabel Said ST4 Clinical Oncology Ninewells Hospital
Topics • Renal Cancer • Bladder Cancer • Prostate Cancer • Testicular Cancer • Penile Cancer
Renal Cancer • 3% of all adult malignancies • 30% presenting with metastatic disease • M>F, ratio 5:3 • 50 – 80 years
Renal Tumours • Benign, example: adenoma • Primary malignant • Renal Cell Carcinoma (RCC) • Lymphoma • Sarcoma • Renal Pelvis Transitional Cell Carcinoma • Secondary malignant (metastatic)
Renal Cell Carcinoma (RCC) – Risk Factors • Smoking • Obesity (especially in women) • Use of phenacetin analgesics • Patients on dialysis, who acquire cystic kidney disease • Occupational risk factors • Leather tanning (TCC – dye and textile industry) • Shoe working • Asbestos expsoure • Genetic risk factors • Von Hippel Lindau disease • Tuberous sclerosis • Adult polycystic disease
Renal Cell Carcinoma – Clinical Presentation • Most are asymptomatic until development of metastasis • Classical triad (19% of cases): • LOIN PAIN • FLANK MASS • HAEMATURIA (painless in TCC) • Fever and sweats • Weight loss • Malaise • Bone pain if metastatic disease • Varicocoele in 2% of males (due to compression of left renal vein) • Paraneoplastic syndrome (symptoms that are the consequence of the presence of cancer in the body, but not due to the local presence of cancer cells)
Renal Cell Carcinoma – Clinical Presentation • Paraneoplastic syndromes • Hypercalcaemia due to PTH-related peptide • Polycythaemia due to EPO-like molecules • Hypertension due to renin • Hepatic dysfunction (unknown mechanism)
Renal Cell Carcinoma - Spread • Local • Adrenal Glands • Renal Veins • Inferior Vena Cava • Gerota’s fascia (anterior to perinephric space) • Perinephric Tissue • Lymphatics • Lymph nodes at renal hilum • Abdominal para-aortic nodes • Paracaval nodes • Blood • Lung • Bone • Soft tissue • Central nervous system • skin
Renal Cell Carcinoma – Investigations and Staging • Abdominal ultrasound scan • CT abdomen – Bosniak 4 part classification uses Hounsefield units to categorise lesions in order of increasing probability of malignancy • CT chest and pelvis • MRI to image the vena cava • Bone scan • FBC • Biochemistry profile including Calcium levels • Renogram if renal impairment present • Renal angiography if partial nephrectomy or palliative embolisation are being considered
Renal Cell Carcinoma - Treatment • Surgery • Radiotherapy (used in Palliative setting) • Biological treatment (used in Palliative setting) • (Chemotherapy unhelpful)
Renal Cell Carcinoma - Surgery • Radical nephrectomy – removal of kidney, adrenal gland, perirenal fat within gerota’s fascia +/- LN dissection • Partial (laparoscopic) nephrectomy – when tumour is small, patients have only 1 kidney • Palliative nephrectomy – • when burden of metastatic disease is small and patient is fit • to improve symptoms such as pain and hypercalcaemia • for patients being considered for immunotherapy • Arterial embolisation • Radiofrequency ablation • Removal of solitary metastasis
Renal Cell Carcinoma - Radiotherapy • Palliative Radiotherapy for symptom control • Bone pain • Haematuria
Renal Cell Carcinoma – Biological Treatment • Cytokine therapy • Interferon α • Interleukin 2 • Signal transduction inhibitors that regulate cell growth, cell proliferation, protein synthesis, and transcription • Tyrosine kinase inhibitors • Sunitinib • Sorafenib • Serine/threonine protein kinase inhibitors - MTOR (mammalian target of rapamycin) • Temsirolimus • Everolimus
Renal Cell Carcinoma - Sunitinib • Oral small molecule TK Inhibitor of Vascular endothelial growth factor (VEGF) and Platelet derived growth factor (PDGF) • First-line for advanced and/or metastatic renal cell carcinoma • Presented at ASCO in 2006: In a phase 3 study - • Median progression-free survival: Sunitinib (11 months) vs Interferon α (5 months) • Secondary endpoints: 28% of patients had significant tumor shrinkage with Sunitinib compared to 5% with Interferon α. • Patients receiving Sunitinib had a better quality of life than interferon α. (N Engl J Med 356 (2): 115–124)
Renal Cell Carcinoma - Sunitinib • Side Effects – “dirty drug” • Thrombocytopenia • Hypertension (+/- proteinuria) • Yellow discoloration of the skin • Fatigue • Gastrointestinal upset (diarrhoea) • Left ventricular dysfunction • Hypothyroidism • Adrenal insufficiency
Bladder Cancer • 6% of cancer cases in males • 2.5% of cancer cases in females • Commoner in Caucasians
Bladder Tumours • Benign, example Papilloma and Leiomyoma • Carcinoma in situ • Primary Malignant • Transitional Cell Carcinoma (90%) • Squamous Cell Carcinoma (5%) • Adenocarcinoma • Small Cell Carcinoma • Sarcoma • Lymphoma • Secondary Malignant • Direct spread from prostate, cervix or vagina • Distant spread
Bladder Cancer – Risk Factors • Smoking • Occupational risk factors • Industrial chemicals such as 2-naphthylamine and acrolein • Chronic urinary stasis (increased risk of squamous metaplasia) • Long term catheter • Bladder stones • Paraplegia • Chronic infection with Schistosomiasis (squamous cell Ca)
Transitional Cell Carcinoma (TCC) • Commonly present in the base of the bladder • Multiple tumours are frequent • Malignant potential: • Low – superficial • High – extension into and beyond muscle wall of bladder • Low Malignant potential TCC are usually curative • High Malignant potential TCC are histologically high grade tumours and >50% of patients will die of their cancers
Transitional Cell Carcinoma – Clinical Presentation • Haematuria • Minimal haematuria with a proven urinary tract infection present in females doesn’t exclude a co-existent cancer • Urgency • Dysuria • Frequency
Transitional Cell Carcinoma – Investigations and Staging • Urinalysis • Flexible cystoscopy • Renal, urinary tracts and bladder ultrasound scan • IVU • CT thorax, abdomen and pelvis • MRI pelvis • Bone scan (bone metastasis present in 5% of cases at presentation)
Transitional Cell Carcinoma – Treatment • Rigid Cystoscopy – Transurethral Resection (TURBT) • Resection of all visible tumour • Additional resection biopsy from the border of the resected area and tumour base for histological assessment of muscle invasion • Radical Cystectomy +/- LN dissection • Radical Radiotherapy (CI: Hydronephrosis, large tumour bulk and multiple tumours) • Neoadjuvant chemotherapy followed by radical cystectomy/ radiotherapy (concurrent chemo-radiotherapy decreases local recurrence rates by 50%)
Prostate Cancer • 2nd most common cause of cancer death in men • Increased screening has led to increased disease incidence • Peak incidence 70 – 75 years • Highest incidence is in Western countries
Prostate Tumours • Benign • Nodular Hyperplasia • Primary Malignant • Adenocarcinoma (>95%) • Transitional Cell Carcinoma • Small Cell Carcinoma • Squamous Carcinoma • Lymphoma • Sarcoma • Secondary Malignant • Direct sspread from Bladder or rectum • Metastatic spread
Prostate Cancer – Risk Factors • Diet rich in animal fat and proteins • Family history
Prostate Cancer – Clinical Presentation • Lower urinary tract symptoms • Haematuria • Perineal pain (rarely) • Bone pain (+/- spinal cord compression) • Lower limb oedema due to lymphadenopathy
Prostate Cancer - Spread • Local • Seminal vesicles • Base of bladder • (spread to rectum is inhibited by the rectoprostatic fascia) • Lymphatics • Pelvic Lymphadenopathy • Para-aortic Lymphadenopathy • Blood • Bone (most common) • Liver (uncommon) • Lungs (uncommon) • (Brain – virtually unknown)
Prostate Cancer – Investigations and Staging • Prostate Specific Antigen PSA (NB: Most aggressive tumours produce little PSA) • Transrectal ultrasound guided systematic sampling • MRI pelvis for extra-capsular involvement, seminal vesicle invasion • CT thorax, abdomen and pelvis (especially for nodal status) • Bone scan
Prostate Cancer - Treatment • Watch and Wait Policy • In patients who are unlikely to develop symptoms • Elderly patients (>75 years) • Younger patients with serious co-morbidities and good- prognosis tumours • Surveillance through regular PSA testing and Digital Rectal Examination
Prostate Cancer – Treatment • Prostate – confined disease • Radical prostatectomy • Interstitial brachytherapy (radioactive iodine seeds) • External beam radiotherapy (+/- adjuvant hormonal therapy) • Locally advanced disease • Neoadjuvant hormone therapy followed by external beam radiotherapy +/- adjuvant hormone therapy • Metastatic Disease • Hormone therapy • Palliative radiotherapy (Bone pain) • Palliative Chemotherapy (Docetaxel/Prednisolone)
Prostate Cancer – Hormone Therapy • Medical castration via LHRH agonist • Example: buserelin, goserelin (given subcutaneously) • with anti-androgens for 2 weeks to prevent transient tumour flare • Contraindicated in patients with • Impending ureteral obstruction • Spinal cord compression • Painful bone metastasis • Anti-androgen therapy • Example: cyproterone, bicalutamide (given orally) • Toxicity: hot flashes, decreased libido, gynaecomastia, nipple pain, impotence and galactorrhea
Testicular Cancer • High cure rate even with metastatic disease • First incidence peak at 25 – 35 years and second at 55 – 65 years • Types: • Germ cell: Seminoma, Teratoma • Non Germ cell: Sex cord tumours, mesenchymal tumours, haemopoetic tumours • Risk factors: • Family history • Subnormal testicular development • Maldescended testicle • Klinefelter’s syndrome • Down’s syndrome
Testicular Cancer Clinical Presentation Spread • Painless testicular swelling ( and raised ßHCG) • Metastatic disease • Fatigue • Weight loss • Shortness of breath due to lung metastasis • Ureteric obstruction and renal failure due to lymphadenopathy • Local (rare) • Lymphatics • Inter-aortocaval lymphadenopathy for right sided tumours • Para-aortic lymphadenopathy for left sided tumours • Pelvic lymphadenopathy • Blood • Lung (common) • Liver (uncommon) • Brain (uncommon) • Bone (uncommon)
Testicular Cancer – Treatment • Testicular-confined disease (example Seminoma): • Orchidectomy and adjuvant radiotherapy to para-aortic lymph nodes or adjuvant chemotherapy with single agent carboplatin • Infradiaphragmatic Lymphadenopathy: • Concurrent chemo-radiotherapy • Metastatic Disease: • BEP chemotherapy (Bleomycin, cisplatin, etoposide) • Relapsed Disease: • High Dose chemotherapy with stem cell support
Penile Cancer • Associated with HPV infection, subtypes 16 and 18 • Squamous Cell Carcinoma • Treatments include: • Penis-preserving surgery with reconstruction • External beam radiotherapy • Brachytherapy • Laser excision • Bilateral Radical Inguinal Lymph Node Dissection • Adjuvant concurrent chemo-radiotherapy • Concurrent chemo-radiotherapy in locally advanced disease • Palliative chemotherapy