Download
1 / 65
780 likes | 1.29k Views
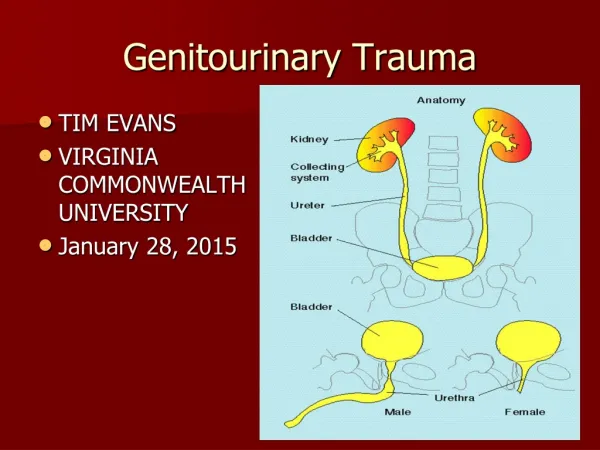
Genitourinary Radiology. Jerry Glowniak, MD Department of Radiology Detroit Receiving Hospital Detroit Medical Center/Wayne State University. Radiological Anatomy: Kidneys and adjacent spaces.

E N D
Genitourinary Radiology Jerry Glowniak, MD Department of Radiology Detroit Receiving Hospital Detroit Medical Center/Wayne State University
Radiological Anatomy:Kidneys and adjacent spaces • The radiological anatomy of the kidneys consists of the cortex, medulla (renal pyramids), renal sinus, and the collecting system. • The kidneys and their adjacent spaces lie in the retroperitoneum in the abdomen and pelvis.
Retroperitoneal Spaces • Radiologically, the retroperitoneum in the abdomen is divided into the perinephric spaces, and the anterior and posterior pararenal spaces. • The retroperitoneal (extraperitoneal) spaces in the pelvis are more complex. The abdominal pararenal spaces continue into the pelvis The perinephric spaces are confined to the abdomen.
The Perinephric Spaces • The largest retroperitoneal spaces. • Contents: the kidneys, adrenal glands, proximal ureters, and perirenal fat. The right and left spaces communicate inferiorly. • Delimited by the renal fascia which has a well-defined anterior component (Gerota’s fascia, anterior renal fascia) and thinner posterior component (Zuckerkandl’s fascia, posterior renal fascia).
Retroperitoneal Spaces: Abdomen • AC – Ascending Colon • DC – Descending Colon • D – Duodenum • K – Kidney • A – Aorta • V – Vena Cava
Anterior Pararenal Space • Single space anterior to the perinephric spaces. • Contents: Pancreas, second and third portions of the duodenum, aorta, inferior vena cava, ascending and descending colon • Anterior boundary: posterior parietal peritoneum. • Posterior boundary: Anterior renal fascia
Posterior Pararenal Spaces • Right and left spaces posterior and lateral to the perinephric spaces. • Contents: Fat • Anterior boundary: posterior renal fascia and lateroconal ligament • Posterior boundary: Transversalis fascia • Anterior to the colon, it is continuous with the properitoneal fat.
Retroperitoneal Spaces: Detailed View • DC – Descending Colon • K – Kidney • PM – Psoas Muscle
Imaging Modalities • Intravenous pyelogram • Computed Tomography (CT) • Ultrasound • Nuclear Medicine • Magnetic Resonance Imaging (MRI) • Plain Film
Intravenous Pyelogram • Gold Standard 20 years ago • Becoming an obsolete technique • Limited views of kidneys • Two dimensional technique • Largely replaced by CT
Normal excretory phase of an IVU (intravenous urogram), 10 minute image. Kidneys are excreting contrast into non dilated calyces (arrows), renal pelvis (p), ureters (*) and bladder (B).
Computed Tomography • Imaging modality of choice for most abnormalities. • Advantages: Fast, widely available, high resolution. • Disadvantages: Radiation, intravenous contrast, less specific than MRI
CECT kidneys, 60 sec (nephrogram phase) , would show renal parenchymal lesions well CECT kidneys; 4 min ( pyelogram phase), showing excretion of contrast into collecting system, would show urothelial lesions well, such as TCC , stones, blood clots
1 2 • CECT scan of abdomen with (1) axial, (2) coronal, and (3) sagittal 3D reconstructions shows multiple cysts (c) of varying sizes in the right kidney in a pattern most consistent with multicystic dysplastic kidney disease. 3
3D reconstructed image from CT scan of the abdomen and pelvis, a CT “IVP”, shows RK (K), a normal ureter (arrows), and the ureter's insertion into the bladder.
Ultrasound • Useful in a wide variety of genitourinary tract abnormalities. • Advantages: Highest resolution, non-invasive, widely available, fast. Real-time assessment of blood flow (color flow imaging). • Disadvantages: Highly operator dependent, images in nonsequential format which makes anatomy more difficult to appreciate.
Nuclear Medicine • Used primarily for obtaining functional information. Limited role in GU imaging. • Advantages: Lower radiation dose than CT, no adverse effects except for radiation. A few unique advantages, e.g. In-111 white blood cell scanning is highly specific for infections. • Disadvantages: Long imaging times, few specific indications, radiation.
Magnetic Resonance Imaging • Increasing role in abdominal/pelvic imaging • Advantages: Many imaging sequences allow highly tailored studies, no radiation, more specific than CT • Disadvantages: Cost, longer imaging times than CT, unable to imaging calcium (renal/ureteral calculi, calcifications)
Plain Films • Useful as a first test in several applications: Renal calculi, emphysematous pyelonephritis, renal size. • Advantages: Cheap, fast, widely available. • Disadvantages: Rarely diagnostic. Further tests required.
Renal Imaging: Radiologic Parameters • In the more commonly used exams in which contrast is given – CT, MRI, IVP – and to a lesser extent, nuclear medicine, images are obtained dynamically. • Three phases defined: Arterial (corticomedullary) 10-20 seconds; Venous (nephrogram) 40-80 seconds; excretory – beyond 80 seconds.
Arterial (corticomedullary) phase – 10 to 20 seconds • Renal artery and vein prominent (arrows) • Cortex clearly differentiated from medulla
Venous (nephrographic) phase 40 – 80 seconds • Vasculature less prominent • The cortex and medulla have the same degree of enhancement
Excretory phase – beyond 80 seconds • Most variable phase • Begins when contrast is seen in the collecting systems
Renal Infections • Pyelonephritis • Renal and perinephric abscess • Emphysematous pyelonephritis • Xanthogranulomatous pyelonephritis
Acute Bacterial Pyelonephritis • Two main routes of infections: reflux and blood borne. • Vesicoureteral reflux, primarily in children, caused by E. coli • Hematogenous, usual cause of infection in adults, caused by Staph aureus. • In uncomplicated infections, imaging usually not necessary.
CT imaging of pyelonephritis • In mild cases, there may be no imaging findings. • The most specific finding is the “striated nephrogram” – alternating stripes or wedges of opacified and nonopacified parenchyma caused by nonhomogeneous edema • Focal defects, global enlargement, and delayed opacification are other less specific findings
Renal/perirenal abscess • CT is highly sensitive, but somewhat nonspecific for abscesses. • The clinical picture of pyuria, flank pain, fever, and tenderness with characteristic findings are usually definitive. • CT shows a low attenuation region without enhancement with a thick, enhancing capsule, adjacent fascial thickening, and fat stranding.
Emphysematous Pyelonephritis • Emphysematous pyelonephritis is a life-threatening infection of the kidneys in which gas is produced. There are 2 types. • Type I: More than one third of the kidney destroyed, no fluid collections. 70% mortality. • Type II: Less than one third of kidney destroyed with fluid collections. Mortality 18%. • Usual treatment: nephrectomy.
Emphysematous cystitis • Gas in the bladder wall usually caused by E. coli. • Occurs in diabetes, bladder outlet obstruction, neurogenic bladder • If no other abnormalities present (abscess, gangrene), usually responds readily to antibiotics
Xanthogranulomatous pyelonephritis • Chronic indolent, renal infection • Renal parenchyma replaced by lipid laden macrophages which can form large masses. • Unusually entire kidney involved. • CT: Low attenuation masses, renal enlargement, usually a calculus (staghorn) present, renal enlargement.
Staghorn Calculus Xanthogranulomatous pyelonephritis
Renal Focal Lesions • Renal cysts are the most common focal renal lesion. • Cysts are ubiquitous with 50% of the population older than 50 having a simple renal cyst. • Simple cysts are easily recognized, but complicated cysts are more difficult to assess in terms of a benign or malignant lesion.
BOSNIAK CLASSIFICATION • I Simple Cyst : Nonoperative • II Septated, minimal calcium described as “egg shell”, thin septa and walls, high-density cysts (> 20HU), non-enhancing : Nonoperative • III Multiloculated, thick walled, dense calcifications; nonenhancing solid component: Renal-sparing surgery • IV Marginal irregularity, enhancing solid component: Radical Nephrectomy
Bosniak II: Faint calcification with hair thin septation , no contrast enhancement
Bosniak III:lobulated, cystic lesionwith irregular, calcifiedseptum
Bosniak IV: Cystic and solid lesion with enhancing solid component: Renal Cell Carcinoma
Angiomyolipoma • Angiomyolipomas are hamartomas containing fat, smooth muscle, and blood vessels • Most are asymptomatic, but large lesions (> 4 cm) may bleed. • 80 % of pts with tuberous sclerosis have AML, usually multiple lesions bilaterally.
AML in tuberous sclerosis • Ultrasound shows multiple, small, hyperechoic foci representing fat containing lesions typical of AML
Oncocytoma • Oncocytomas are benign renal tumors with no metastatic potential but are indistinguishable radiographically from Renal Cell Carcinoma (RCC) • Biopsy is of little use because RCC can contain elements of oncocytoma • If there is a strong suspicion that the mass in question is benign, a renal sparing procedure is an option