Download

1 / 51
540 likes | 1.04k Views
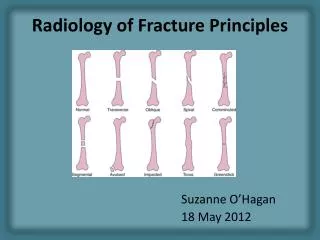
Principles of Fracture Treatment. Definition of Fracture. It is disruption of bone continuity. Although most of #s occur as a result of a single episode by a force powerful enough to fracture a normal bone, there are 2 types of # in which this is not so : Pathological fract.

E N D
Definition of Fracture • It is disruption of bone continuity. Although most of #s occur as a result of a single episode by a force powerful enough to fracture a normal bone, there are 2 types of # in which this is not so : • Pathological fract. • Stress fract.
Pathological fracture : It is one in which a bone is broken through an area weakened by pre-existing disease , & by a degree of force that would have left normal bone intact e.g osteoporosis , O.M. , bone tumours.
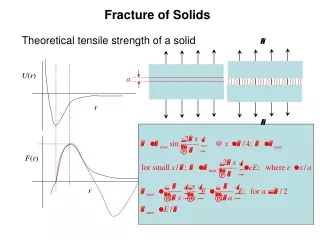
Stress fracture : Bone , like other materials , reacts to repeated loading . On occasion , it becomes fatigued & a crack develops e.g military installations , ballet dancers & athletes.
Diagnosis • Clinical picture • Radiography
Clinical Features of Fracture • History of trauma • Symptoms & signs: 1. Pain & tenderness 2. Swelling 3. Deformity 4. Crepitus 5. Loss of function 6. Abnormal move. 7. N.V. injuries
Radiographic Findings • Plain x-ray: should show joint above & joint below , in at least 2 views , special views on request. • C.T. • MRI : It is not helpful in fract. diagnosis other than delineating associated injuries to the CNS , S.T. disruption or occasionally fatigue fract.
Anat. Location Direction of fract. Line Wherther the fract. Is linear or comminuted Condition of overlying S.T. Mechnism of injury AO classification Fracture Classification
AO Classification • A : Simple fract. • B : Wedge fract. • C : Complex fract.
AO Classification B= wedge fract. B3 wedge fract fragmented wedge
Mechanism of Injury Classification • Direct trauma • Indirect Trauma
Direct trauma : • Tapping fractures • Crushing fractures • Penetrating fractures - High velocity missiles > 2500 f/s - Low velocity missiles < 2500 f/s
Indirect Trauma : • Traction or tension fract. • angulation fract. • Rotational fract. • Compression fract.
Fracture Management • Emergency care – (splinting) • Definitive fracture treatment • Rehabilitation
Emergency care – (splinting) • Splint them where they lie. • Adequate splinting is desirable , why ? • Types of splints : - improvised - conventional
Definitive fracture treatment The goal of fracture treatment is to obtain union of the fracture in the most anatomical position compatible with maximal functional return of the extremity. • Conservative • Operative
Conservative • Reduction : if displaced under G.A. the sooner the better. steps :- traction , align (which fragment), reverse mechanism of injury. • Immobilization : POP cast , slab , traction (fixed or balanced). • Rehab.
CLOSED, UNDISPLACED CLOSED, REDUCIBLE CONSERVATIVE TREATMENT 2- CAST Above Knee Below Knee
Operative • ORIF (open reduction internal fixat.) • Percutineous pinning • External fixation
Indications of ORIF - absolute - relative
Types of Internal Fixation - Pin & wire fixat. - Screw fixat. - Plate & screws fixat. - Intra-medullary fixat.
Plate & screws fixat. Functional types: • Compression plates • Neutralization plates • Buttress plates • Bridge plates • LC- DCP • Liss plates • Locking plates & screws
Intra-medullary fixat. • Centro-medullary - Unlocked -Interlocking(static – dynamic – double locked) • Condylocephalic • Cephalomedullary
CONTRAINDICATIONS TO SURGICAL REDUCTION AND STABILIZATION Situations in which there is a high probability for failure with operative treatment are as follows: 1. Osteoporotic bone that is too fragile to allow stabilization by internal or external fixation. 2. Soft tissues overlying the fracture or planned surgical approach of such poor quality because of scarring, burns,active infection, or dermatitis . 3. Active infection or osteomyelitis. 4. Fracture comminution to a degree that does not allow successful reconstruction. This is most commonly seen in severe intraarticular fractures. 5. General medical conditions that are contraindications to anesthesia are generally contraindications to the surgical treatment of fractures. 6. Undisplaced or stable impacted fractures in acceptable position do not require surgical exposure or reduction. 7. Inadequate equipment, manpower, training, and experience.
Rehabilitation • When ? • How ?
External fixat. • Advantages. • Disadvantges. • Complications. • Indications.