Download
1 / 11
110 likes | 122 Views
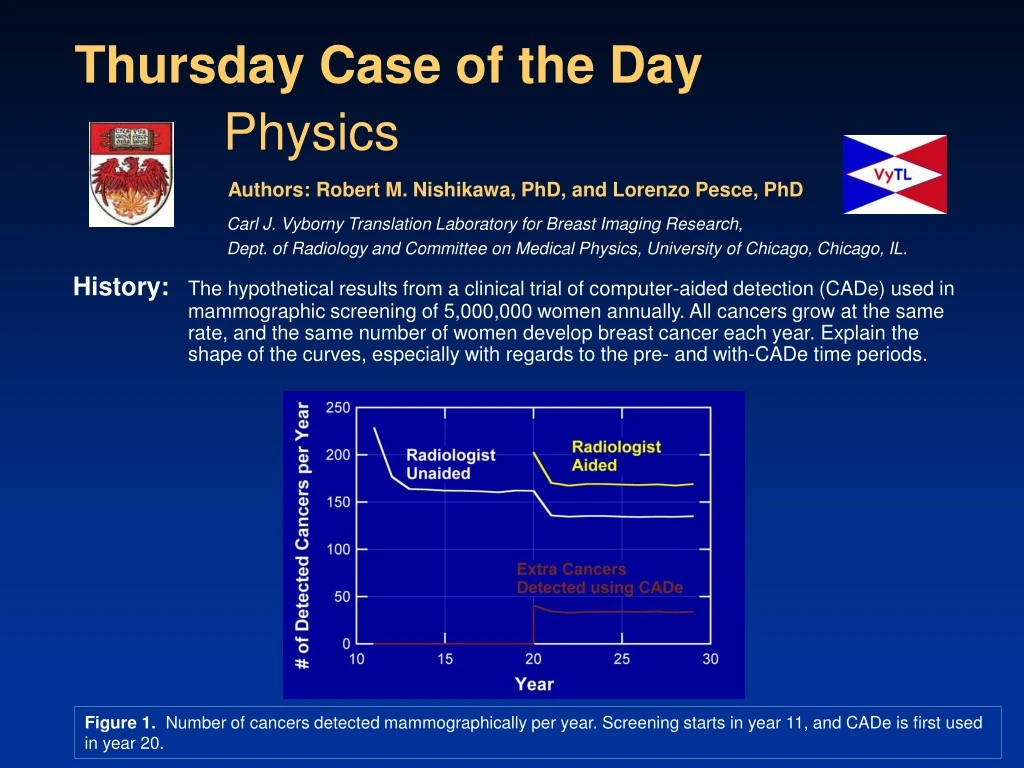
This article examines the results of a hypothetical clinical trial of CADe in mammographic screening of 5,000,000 women. The study explores the shape of the curves and the impact of CADe on cancer detection rates.

E N D
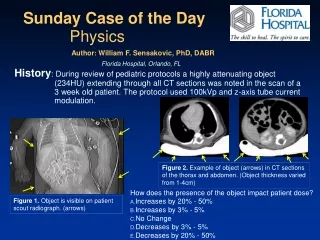
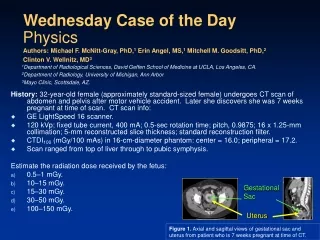
History:The hypothetical results from a clinical trial of computer-aided detection (CADe) used in mammographic screening of 5,000,000 women annually. All cancers grow at the same rate, and the same number of women develop breast cancer each year. Explain the shape of the curves, especially with regards to the pre- and with-CADe time periods. Thursday Case of the Day Physics Authors: Robert M. Nishikawa, PhD, and Lorenzo Pesce, PhD Carl J. Vyborny Translation Laboratory for Breast Imaging Research, Dept. of Radiology and Committee on Medical Physics, University of Chicago, Chicago, IL. Figure 1. Number of cancers detected mammographically per year. Screening starts in year 11, and CADe is first used in year 20.
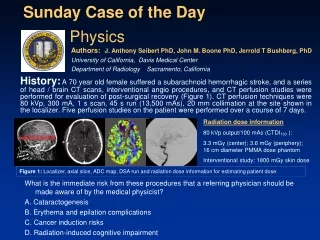
Findings:Increase in cancers detected when screening is introduced and when CADe is introduced (prevalence screens). Figure 2. The arrows indicate prevalence screen with mammography (years 11–13) and with CADe (years 20–21).
Findings:Decrease in cancers detected by the radiologist in the unaided reading condition when CADe is used (years 21–29) compared to when CADe is not used (years 14–19), excluding the prevalence screening periods. Figure 3. The arrow indicates that there is a time period where there is a decrease in the number of cancers detected by the radiologist that were detected unaided (ie, detected before reviewing the CADe output) per year (years 21–29).
Findings:The number of cancers detected per year increases slightly when CADe is used (years 21–29) compared to when CADe is not used (years 14–19), excluding the prevalence screening periods. Figure 4. The two white arrows indicate the size of the increase in the number of cancers detected by the radiologist when CADe is used compared to before CADe was implemented (after the prevalence CADe screen).
Findings:The increase in the number of additional cancers detected per year because CADe is used (approximately 40) is larger than the increase in the number of cancers detected per year (approximately 10). Figure 5. The lower set of white arrows indicates the number of extra cancers detected by the radiologist when CADe is used (after the prevalence CADe screen).
Diagnosis:As measured by the change in the cancer detection rate, CADe is not effective in screening mammography. However, there is a large increase in the number of additional cancers detected each year because CADe is used. That is, CADe can reduce the “miss” rate of radiologists, thereby detecting cancers at an earlier stage, but this is not evident from measuring the cancer detection rate.
Discussion:Just as when screening is introduced, when CADe is initially implemented, the cancer detection rate is elevated initially (prevalence screen), and then the lower incidence rate is reached. The initial increase when screening is introduced is because there are cancers in the patient population that are detectable by mammography but are clinically occult. When screening is initiated, these cancers are found, but after a short time (3 years in this example), these types of cancers are no longer present. With CADe, there are cancers in the patient population that will be mammographically detectable but will be overlooked by the radiologist. CADe can help detect these cancers, so when initially implemented, the cancer detection rate will be elevated. Figure 2. The arrows indicate prevalence screen with mammography (years 11–13) and with CADe (years 20–21).
Discussion:After CADe is introduced, some of the mammographically detectable cancers that would have been overlooked are detected because CADe is used. The amount depends on the sensitivity of the CADe system and the radiologist’s ability to recognize when CADe has detected a missed cancer. Once potentially overlooked cancers are detected when using CADe, they are no longer “available” to be detected in subsequent years. Therefore, the number of cancers detected unaided (ie, before looking at the CADe output) by the radiologist per year is lower than the number detected before CADe is introduced. Figure 3. The arrow indicates a decrease in the number of cancers detected by the radiologist that were detected unaided (ie, detected before reviewing the CADe output) per year (years 21–29).
Discussion:The cancer detection rates before and after the introduction of CADe (excluding the prevalence years) are nearly identical. This is because all breast cancers in the patient population will eventually be detected, either mammographically or as an interval cancer (in this example, it is assumed that there are no other causes of death). Therefore, in a fixed patient population, the cancer detection rate before and after CADe is implemented cannot be different, except for the small number of CADe-detected cancers that would have been detected as an interval cancer if CADe were not used. Figure 4. The two white arrows indicate the size of the increase in the number of cancers detected by the radiologist when CADe is used.
Discussion:Although the cancer detection rate does not increase appreciably after CADe is initiated (~10), the number of additional cancers that are detected because CADe is used can be substantial (~40). This emphasizes that the goal of CADe is to find cancers at an earlier stage, not to find more cancers per se. In terms of measuring the effectiveness of CADe, measuring the change in the cancer detection rate will not be useful. Measuring the number of additional cancers is more indicative of the effectiveness of CADe, but this method suffers from significant biases that make it difficult to interpret the results. Figure 5. The lower set of white arrows indicates the number of extra cancers detected by the radiologist when CADe is used (after the prevalence CADe screen).
Discussion:Since the goal of CADe is to find cancers at an earlier stage and not to find more cancers per se, the number of cancers detected per year is not a true indicator of the effectiveness of CADe. A more appropriate end point for measuring the effectiveness of CADe is to measure the average size of detected cancers. That is, CADe should allow for cancers to be detected earlier, and therefore the mean size of the detected cancers should decrease when CADe is used. This exhibit demonstrates that the change in cancer detection rate is not an appropriate means to measure the effectiveness of CADe.