Download
1 / 82
820 likes | 834 Views
Discover what psoriasis is, its causes, and the various symptoms and types of this common autoimmune skin disease. Learn about available treatment options and how to manage the condition.

E N D
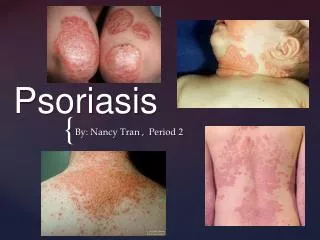
Psoriasis Lianjun Chen Huashan Hospital
WHAT IS PSORIASIS? • A common, life-long, genetic, autoimmune skin disease • Characterized by well circumscribed areas of thick, red, scaly skin • From the Greek “psoros” meaning “rough, scabby” • Term first used (along with “lepra”) by Hippocrates (460-377 B.C.) in Corpus Hippocraticum • von Hebra first to distinguish psoriasis from leprosy in 1841
Morbidity rate • Natural population: 0.1%~3%. Estimated 1.25 hundred million patients in the world • China(1984): 0.123%. • European country: 1.5%-3%. • America: 2.6%. • Hongkong:0.3%(2005 )
Prevalence • Equal frequency in males and females • May occur at any age from infancy to the 10th decade of life • First signs of psoriasis • Females mean age of 27 years • Males mean age of 29 years
Prevalence • Two Peaks of Occurrence • One at 20-30 years • One at 50-60 years • Psoriasis in children • Low – between 0.5 and 1.1% in children 16 years old and younger • Mean age of onset - between 8 and 12.5 years
Etiopathogenisis 1.Theory of heredity Family positive of psoriasis is 4~91%, 11.9~32% in china Concordance rate in twins: monozygotic twins> binovular twins High frequency in HLA-A1,B17,Cw6,DR7, a multifactorial inheritance disease
PSORS9 4q31-q32 zhang Xuejun,2002
Psoriasis, an inherited disease If you have psoriasis, what is the risk to: • Your unrelated neighbor? About 2% • Your sibling? 15-20% • Your identical twin? 65-70% • Your child? 25%-50%
Etiopathogenisis 2.Theory of infection bacterial infection(esp.streptococcus) fungal infection bacteria fungi (streptococcus、superantigen) (yeast fungus) lymphocytes activated alternative complement pathway clonal proliferation functional disorder of immune system
Etiopathogenisis 3.Abnormal immune function : cellular immunity function reduce partly early skin lesions are infiltrated predominantly by lymphocytes autoantibody deposit in the horny layer Th1/Th2 disequilibrium theory(Th1 dominant skin disease)
Etiopathogenisis 4.Dysmetabolism: cAMP metabolic block of arachidonic acid、 cGMP polyamines shortened epidermal cell transit time, hyperplasia 5.others: psychosis,neuroendocrine,climate,medicine , et al may induce or aggravate the disease.
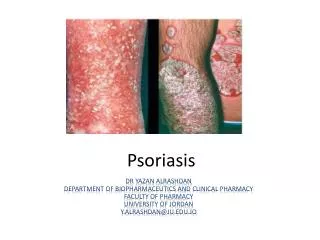
Clinical Presentation • Erythematous papules/patches/plaques with silvery scales • Symmetric • Pruritic/ Painful(sometimes) • Pitting Nails • Arthritis in 10-20% of patients • Exacerbate in winter ,improve in summer
Clinical Types • Psoriasis Vulgaris • Psoriasis Arthropathica • Psoriasis Pustulosa • Psoriasis Erythrodermica
Psoriasis Vulgaris • red papule/plaque • silvery white scales • film phenomenon • pinpoint bleeding Auspitz’s sign
P S O R I A S I S Disorganized N O R M A L STRATUM CORNEUM Neutrophil accumulation STRATUM GRANULOSUM STRATUM SPINOSUM Immaturity Proliferation STRATUM BASALE DERMIS
CLASSIC ANATOMIC LOCATIONS FOR PSORIASIS • Scalp (80%) • Elbows (78%) • Legs (74%) • Knees (57%) • Nails (10-55%) • Gluteal cleft • Palms/soles (12%)
Guttate Psoriasis • Characterized by numerous 0.5 to 1.5 cm papules and plaques • Early age of onset • Most common form in children • Streptococcal throat infection often a trigger • Spontaneous remissions in children • Often chronic in adults
Rhagades and thickness scales in palms and soles
Psoriasis of genitalia scantiness of scale
Flexural psoriasis (Psoriasis of vulvae,red plaque with little scaling)
PSORIATIC NAIL CHANGES • Onycholysis • “Oil drops” • “Salmon patches” • Pitting • Subungual debris • Onychodystrophy • Splinter hemorrhages
TRIGGERS FOR PSORIASIS • Direct skin injury (Koebner phenomenon) • Discontinuation of systemic corticosteroids • Cold weather • Streptococcal pharyngitis • Emotional stress • Alcohol intake • Smoking • HIV • Medications
DRUGS THAT CAN EXACERBATE PSORIASIS • *Beta blockers • *Lithium • *IFN-alpha • Antimalarials • ACE inhibitors • *Rebound with withdraw of prednisone and cyclosporine
STAGE OF PSORIASIS • Active stage: large amounts of new lesions,red and pruritus • Resting stage: dark red lesions without new eruption • Regression stage: erythema fade, flatten and disappear
Koebner Phenomenon • Mechanical injury,insect bite,cold injury, sun shine et al • Normal skin of patients in active stage express typical new lesions • Clinical significance: suggest disease in active stage
Course of psoriasis • exacerbate in winter ,improve in summer • chronic and persistent • clear spontaneously, recur frequently
Diagnosis and differential diagnosis • Diagnosis: lesions,types and stages • Differential diagnosis: • pityriasis rosea • secondary syphilis • Seborrheic dermatitis • chronic eczema
Generalized Pustular Psoriasis • Unusual manifestation of psoriasis • Can have a gradual or an acute onset • Characterized by waves of pustules on erythematous skin often after short episodes of fever of 39˚ to 40˚C • Weight loss • Muscle Weakness • Hypocalcemia • Leukocytosis • Elevated ESR