Download
1 / 21
260 likes | 807 Views
Lower Urinary tract infection:. Cystitis, Urethritis, and Prostatitis in men. Cystitis : is the inflammation of urinary bladder caused by microbial invasion and colonization. Hemorrhagic cystitis : - is characterized by large quantities of visible blood in the

E N D
Lower Urinary tract infection: Cystitis, Urethritis, and Prostatitis in men. Cystitis: is the inflammation of urinary bladder caused by microbial invasion and colonization. Hemorrhagic cystitis : - is characterized by large quantities of visible blood in the urine. - Etiology: bacterial causes or adenovirus. -Acute cystitis in woman presents with lower-tract irritative symptoms such as dysuria, frequent urination, and urgency (need to void immediately). -Some cases also experience gross Hematuria.
n Urethritis : It is the inflammation of urethra due to microbial invasion. Most cases of Urethritisare sexually transmitted. If vaginal discharge or irritation are present; alternative diagnosis of Vaginitis should be considered.
N Bacterial prostatitis: -inflammation of prostate in men mainly caused by bacterial invasion. -Acute prostatitis: high fever, and pelvic pain. -Chronic bacterial prostatitis:(Rare infection): usually characterized by recurrent acute cystitis from relapses of bacteria persisting in the prostate (Prostate stones).
Causes of Bacterial Cystitis and Prostatitis: Cystitis: 1- Escherichia coli : 80-85% of cases. 2-Staphylococcus saprophyticus: 5-15% of cases. 3- Other genera of Enterobacteriaceae: Lactose fermenters: Klebsiella, Enterobacter, and Citrobacterspecies. Urease producing organisms: Proteus mirabilis and Morganellamorganii. Others: Serratia species. 4-Pseudomonas aeruginosaandEnterococcus faecalis. 5-Candida albicansandCandida tropicalis. Acute Prostatitis: Staphylococcus aureus and E. coli.
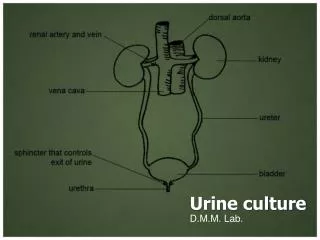
Diagnosis of Urinary tract infection: Collection of Clinical Specimens: Urine specimens: A- Midstream catch urine: One to Ten ml: Should be collected in sterile urine container , the first portion must be discarded to avoid contamination with urethral and vaginal bacteria. B- Catheterized Urine: One to Ten ml Should be collected in sterile urine container. C- Suprapubic Urine: One to Ten ml Aspirated from urinary bladder by fine needle collected in sterile anaerobic tube. ( young babies, children, obstruction cases).
Isolation of Pathogens and Calculation of Colony forming units (CFU/ml): Urine specimens should be cultivated on: 1-Enriched media: Blood agar (General media for isolation of all types of bacteria). 2-Differential or Selective media: MacConkey’s or CLED (EMB): for Enterobacteriaceae. Colony forming units: -Is the original number of bacterial cells present in the clinical Specimen per one milliliter. - Calibrated loop carry only one microliter.
N Urine Specimens should be cultivated by 1-Network Streaking method : (Calibrated Loop) (quantitative method for calculation of CFU/ml). 2-Four quadrant streaking method: (Calibrated Loop). (Semi-quantitative methodfor isolation of different species).
N Significant bacteriuria and Colony forming unit Cutoff value: Significant bacteriuria: Is the isolation of microbes with a specific pathogenic dose cutoff value from urine Specimen in presence of signs and symptoms of UTI (Pyuria and dysuria). The CFU Cutoff value is calculated to be : For Midstream catch urine = (5*104)- 105CFU/ml For Catheterized Urine = 102CFU/ml For Suprapubic Urine = Any growth. In Immunocompromised Patients = Any growth.
N Asymptomatic Bacteriuria: Is the presence of significance or non-significance CFU of bacteria in urine without signs and symptoms of UTI. It is mainly associated with: 1-Contamination of urine (during collection of specimen). 2-Immunocompromised host. Other Cultivation methods: 1-Plate-spreading methods: For antibiotic sensitivity test. 2-Microbroth dilution method: For calculation of therapeutic dose of antibiotic.
Identification of E. coli: -Some strains of uropathogenicE. coliare verotoxin producers. -All strains are oxidase negative and catalase positive. -Metallic green sheen on EMB agar. -UropathogenicE. coli species are indole positive.
Identification of Proteus species: (Non-Lactose fermenter) All species are Gram’s negative bacilli that illustrate swarminggrowth on blood agar. All are H2S producers and urease positive.
Isolation of Pseudomonas and Serratia species: -All species of Pseudomonas produce water -soluble Exopigmenton nutrient agar.(greenish yellowish pyoverdin) -All species are oxidase positive. -Serratia marcescens produces a deep red pigment (water- insoluble) at 25°C, but does not produce pigment at 37°C. Serratia marcescens Pseudomonas
Isolation of Gram’s positive Cocci: 1-Staphylococcussaprophyticus. 2-Enterococcusfaecalis. 3- Staphylococcus aureus.
N -Staphylococcus saprophyticusspecies are Mannitol fermenters and Novobiocinresistant. -Enterococcus faecalisspecies grow with black discoloration on bile esculine salt agar.
Parasitic infection of urinary system: Schistosomiasis: Classification (phylum): Trematoda. Classification according to morphology: Flattened non-segmented unisexual flukes. Schistosoma hematobium: • Found in Middle East,and Africa. • Definitive host: Man • Intermediate host: Snails. • It causes Urinary bilharziasis (female deposits eggs in the pelvic plexus of venous circulation).
Stages of Schistosomiasis: 1-Incubation period: (acute Schistosomiasis 6-12 Weeks) : -This stage is characterized by skin irritation . -Late in the incubation period: A- Enlarged liver, fever, headache, anorexia, loss of weigh. B- CBC shows Eosinophilia. 2- Stage of egg deposition: (1- 5 years after infection). Urinary bilharziasis : Dysuria with terminal hematuria. Schistosoma hematobiumova passes in urine Oval 140x50 µm with terminal spine.
N 3-Stage of complication: -Due to a fibrosis around the eggs in bladder, liver and lung and granulomatous reactions. - Cystitis and obstruction of bladder. Late stage: - Pyonephrosis and hydronephrosis. - Risk for urinary bladder carcinoma.
Clinical Case: At 67 years of age, Mr. H underwent a transurethral prostatectomy For cancer of the prostate. Because of concern about postoperative bleeding from straining during urination, he had a catheter placed into the bladder. Three days later, Mr. H developed a urinary tract infection with low-grade fever, some pain, and pyuria. Quantitative urine culture counts 3*105 CFU/ml of urine. The microbe was Gram’s negative lactose fermenter bacilli with indole positive reaction. Physicians were able to control the infection with gentamicin therapy.
N This case raises several questions: 1-What is the type of UTI; Hospital or Community-Acquired? 2-How did Mr. H acquire this infection? 3-does this UTI has a significant diagnostic reference. Why? 4-What is the causative agent? 5-How can you confirm your answer? 6-How can this scenario be prevented?