Download
1 / 19
190 likes | 199 Views
This study evaluates the AFP model in patients with low-risk recurrence profiles to support its use in candidate selection for liver transplants. The research explores if the model can predict recurrence risk and post-transplant survival better than standard Milan criteria based on pre-transplant data. Data was gathered from 40 LT centers in France, Italy, and Latin America from 2000 to 2012, focusing on recipient characteristics, tumor burden, and AFP levels at listing. The study aims to improve candidate selection and transplant outcomes, enhancing decision-making processes.

E N D
O-31“Evaluation of the AFP model in patients with low risk recurrence profile: further evidence to support its inclusion for candidate selection". Authors:Federico Piñero1,2*, Charlotte Costentin3*, Andrea Notarpaolo4*, Ilka F Boin5, Karim Boudjema6, Cinzia Baccaro7, Luis G Podestá1,2, Philippe Bachellier8, Giuseppe Maria Ettorre9, Jaime Poniachik10, Fabrice Muscari11, Fabrizio Dibenedetto12, Sergio Hoyos Duque13, Ephrem Salame14, Umberto Cillo15, Adrián Gadano16, Claire Vanlemmens17, Stefano Fagiuoli18, Fernando Rubinstein19, Patrizia Burra20, Marcelo Silva1,2, Christophe Duvoux21 and the French-Italian-Latin American collaborative group for HCC and liver transplantation. Afilliations:1- Hospital Universitario Austral, Facultad de Medicina de la Universidad Austral, Argentina. 2- Latin American Liver Research Educational and Awareness Network. 3- Gastroenterology, Hepatology and Transplant Unit, CHU Grenoble-Alpes, Grenoble, France; 4- Arcispedale Santa Maria Nuova, Reggio Emilia, Italy. 5-Hospital das Clinicas UNICAMP Campiñas, Brazil; 6-Department of Hepatobiliary and Digestive Surgery, Pontchaillou Hospital Rennes 1 University, Rennes, France; 7- Lanciano’s Hospital, Chieti, Rome, Italy; 8- Digestive Surgery Unit, CHU de Strasbourg, Strasbourg, France; 9-Ospedale San Camillo di Roma, Rome, Italy; 10-Hospital Clínico de la Universidad de Chile, Santiago, Chile; 11- Digestive Surgery and Transplant Unit, HôpitalRangueil, Toulouse, France; 12- Hepato-Pancreato-Biliary Surgery and Liver Transplantation Unit, Department of General Surgery, University of Modena and Reggio Emilia; 13-Hospital Pablo Tobón Uribe y Grupo de Gastrohepatología de la Universidad de Antioquía, Medellín, Colombia; 14-Digestive Surgery Unit, CHU de Tours, Tours, France; 15- Hepatobiliary Surgery and Liver Transplant Unit, Padova University Hospital; 16-Hospital Italiano de Buenos Aires, Argentina; 17-Hepatology Unit, Hôpital Juan Minjoz, Besançon, France; 18- Gastroenterology, Hepatology and Transplantation, Papa Giovanni XXIII Hospital, Bergamo, Italy; 19-Instituto de EfectividadClínica y Sanitaria (IECS), Buenos Aires, Argentina. 20- Multivisceral Transplant Unit, Department of Surgery, Oncology and Gastroenterology, Padova University Hospital; 21- Hospital Henri Mondor, University of Paris-Est, Creteil, France. Corresponding author, contact information Federico Piñero, MD MSCE. E-mail: fpinerof@cas.austral.edu.ar
Background • The AFP model, which includes number of nodules, size of the largest nodule and serum AFP values before transplantation [1], improves candidate selection for LT both within and beyond Milan criteria [2-3]. • However, the final recurrence risk assessment and survival needs to be revised based on explant pathology data [4-6]. • It has been shown that AFP values correlate with dedifferentiated tumors and mvi at explant pathology analysis [2-5]. However, these findings are usually assessed after transplantation. • Consequently, it is uncertain whether pre-transplant selection criteria remain robust in patients with no extensive tumors, without mvi or dedifferentiated tumors at explant pathology. [1] Duvoux C, et al. Gastroenterology 2012;143:986–994.e3. doi:10.1053/j.gastro.2012.05.052. [2]Notarpaolo A, et al. J ofHrepatology 2017 [3] Piñero F, et al. LiverInternational 2016;10:35–43. doi:10.1016/S1470. [4] Costentin CE, et al. IntJnlLab Hem 2015;38:1515–25. doi:10.1111/j.1538-7836.2010.03994.x. [5]Decaens T, et al. LiverInternational 2011;31:792–801. doi:10.1111/j.1478-3231.2010.02425.x. [6]Mazzaferro V, et al. Lancet Oncology 2009;10:35–43. doi:10.1016/S1470.
Aims • We hypothesized that the AFP model might also work in patients without the aforementioned explant pathology risk factors. • Therefore, we sought to explore in patients with a “low-risk” recurrence profile at explant pathology, if the AFP model at listing could still discriminate the risk of recurrence and post-transplant survival better than Milan and other composed criteria. This study was registered on an open public registry (NCT03775863; www.clinicaltrials.gov).
Methods I • Multicenter cohort study conducted in 40 different LT centers from France, Italy and Latin Americaincluding consecutive adult patients with HCC who underwent LT (2000-2012). • Common exposure variables: • Recipient characteristics, pre-transplant tumor burden and α-fetoprotein (AFP) serum levels, all of them obtained at listing. • Milan criteria was the common standardized patient selection in all centers. • Bridging therapies prior to transplantation were also registered. • In patients receiving bridging therapies during the waiting list period, last available radiologic tumor staging and AFP values following these procedures were also registered. • Explant-based pathology findings: common standardized macro and microscopic evaluation. • Presence of macro or mvi, and tumor differentiation (Edmonson-Steiner grading system). • Necrotic nodules were also measured including necrotic and viable tumor diameter. • The Up-to seven criteria were also applied in the explanted liver specimen [6]
or Milan Criteria Mazzaferro V, et al. Nejm 1996 <3 nodules, <3 cm 1 nodule <5 cm AFP model criteria + AFP + Duvoux C, et al. Gastroent 2012 AFP ng/ml ≤100 = 0 points 101-1000 = 2 points >1000 = 3 points Largest tumor diameter ≤3 cm = 0 points 3-6 cm = 1 point >6 cm = 4 points Nº HCC nodules 1-3 = 0 points ≥4 = 2 points
Methods II • Study end-points: • cumulative incidence of recurrence; • overall patient survival since transplantation; HCC-specific survival. • We performed different steps for the analysis: • Selection of patients with an explant-based “low-risk” recurrence profile by a Cox regression multivariable model. • Comparison between Milan and AFP model at listing and their association with HCC recurrence and post-LT survival competing risk regression analysis: competing events for HCC recurrence (any cause of death prior to HCC-R) and for HCC-specific survival (non-HCC deaths). • Models performance: Harrells c-statistic, Somers’ D: Milan vs AFP model vs Metroticket v2.0 • Sensitivity analysis: “low-risk” recurrence profile based on another explant-based model (RETREAT score). This study was registered on an open public registry (NCT03775863; www.clinicaltrials.gov).
Results n=1270
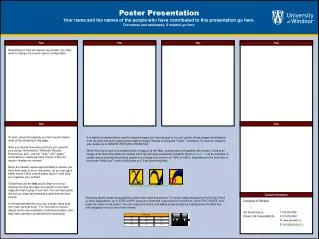
The AFP modelstratifiedsurvival and HCC recurrenceamongpatients within and beyondMilancriteria in theoverallcohort. BeyondMilan+ AFP ≤2 pts[74.7% (CI 67.5-81.0%)] WithinMilan+ AFP ≤2 pts[72.2% (CI 69.2-75.1%)] Beyond+ AFP >2 [40.2% (CI 30.8%-50.1%)] WithinMilan+ AFP >2 pts [51.4% (CI 41.5-61.2%)] WithinMilan+ AFP >2 [29.2% (CI 16.9%-44.1%)] BeyondMilan+ AFP >2 pts [43.7% (CI 29.4-58.8%)] BeyondMilan+ AFP ≤2 [10.9% (CI 6.7%-16.5%)] WithinMilan+ AFP ≤2 [10.7% (CI 8.7%-12.8%)]
Explantpathology variables associatedwith HCC-Recurrence. Cox regressionmultivariable.
Basedonthepresence of at leastone of thesepathologyexplant-based variables, twopopulationswithdifferentrisk of R-HCC wereidentified.
Overall survival and recurrence among “Low vs High-risk” explant-based profile patients 5-yr Recurrencerate <10% “Low-riskprofile” “Low-riskprofile”
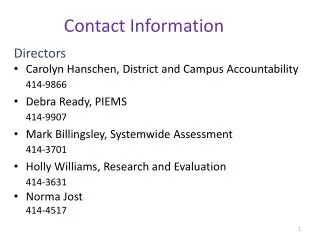
HCC-specific survival among “Low-risk” explant-based profile patients according to Milan criteria and AFP model at listing AFP model MILAN aSHR 0.32 (0.12;0.85)
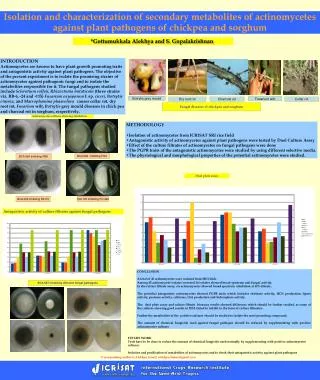
Cumulative HCC recurrenceamong “Low-risk” explant-basedprofilepatientsaccording to Milancriteria and AFP model at listing(Competingriskregressionanalysis) AFP model MILAN aSHR 0.73 (0.33;1.64) aSHR 0.35 (0.13;0.92) • Moreover, in pts with bridging therapies, last tumor imaging assessment, the AFP model was associated with risk of recurrence with a • SHR of 0.26 (CI 0.09;0.68; P=0.006), whereas Milan criteria was not SHR 0.79 (95% CI 0.35;1.77; P=0.57).
Model’s performance: HCC recurrencein patientswithlow-riskexplant-basedprofile Note: *Harrells’c and Somers’ D-indexforeachmodel and P valueswhencompared to the AFP score.
Sensitivityanalysis. “Low-risk” profile according to RETREAT score (another explant-based model) The AFP model assessed at listing could stratify two recurrence risk populations even according to the RETREAT score as a selection tool for categorizing low risk of recurrence with a cumulative SHR of 0.23 (CI 0.07;0.76; P=0.016). Kappa agreement between our selection process and the RETREAT score was 0.57 (P<0.0001).
Summary & Conclusions • Our study highlights the role of the AFP model as a predictor of post LT survival and recurrence in patients who received a liver transplantation for hepatocellular carcinoma (HCC). • The AFP model at listing could better stratified survival and recurrence after transplantation when compared to Milan criteria, even in patients with an explant-based low risk profile for HCC recurrence. • Our results showed further evidence to support the AFP model as inclusion criteria for transplant candidate selection.
Ackowledgements • To everyco-autor whoparticipated in thiscohortstudy. • To thepatientsincluded in thisstudy. France: Karim Boudjema, Philippe Bachellier, Filomena Conti, Olivier Scatton, FabriceMuscari, EphremSalame, Pierre Henri Bernard, Claire Francoz, Francois Durand, SébastienDharancy, Marie-lorraine.Woehl, Claire Vanlemmens, Alexis Laurent, Sylvie Radenne, JérômeDumortier, Armand Abergel, Daniel Cherqui, Louise Barbier, Pauline Houssel-Debry, Georges Philippe Pageaux, Laurence Chiche, Victor Deledinghen, Jean Hardwigsen, J Gugenheim, M altieri, Marie Noelle Hilleret, Thomas Decaens, Christophe Duvoux. Latin America: Paulo Costa, Elaine Cristina de Ataide, Sergio Hoyos Duque, Sebastián Marciano, Margarita Anders, Adriana Varón, Alina Zerega, Jaime Poniachik, Alejandro Soza, Martín Padilla Machaca, Josemaría Menéndez, Rodrigo Zapata, Mario Vilatoba, Linda Muñoz, Martín Maraschio, Luis G Podestá, Lucas McCormack, AdrianGadano, Ilka SF FatimaBoin, Jose Huygens Parente García. Italy: Andrea Notarpaolo, GiuliaMagini, Lucia Miglioresi, Martina Gambato, Fabrizio Di Benedetto, Cecilia D’Ambrosio, Giuseppe Maria Ettorre, AlessandroVitale, Patrizia Burra, Stefano Fagiuoli, UmbertoCillo, MicheleColledan, DomenicoPinelli, Paolo Magistri, Giovanni Vennarecci, Marco Colasanti, Valerio Giannelli, Adriano Pellicelli, CiziaBaccaro.
Survival and HCC recurrence among “High-risk” patients according toMilan criteria at listing
Survival and HCC recurrence among “High-risk” patients according toAFP model at listing