Download
1 / 46
500 likes | 1.01k Views
OXYHEMOGLOBIN DISSOCIATION CURVE. Dr. S. Parthasarathy MD., DA., DNB( anaes ), MD ( Acu ), Dip. Diab . DCA, Dip. Software statistics PhD ( physio ) Mahatma Gandhi medical college and research institute , puducherry – India. HOPE THIS WOULD BE A VERY USEFUL LECTURE

E N D
OXYHEMOGLOBIN DISSOCIATION CURVE Dr. S. Parthasarathy MD., DA., DNB(anaes), MD (Acu), Dip. Diab. DCA, Dip. Software statistics PhD (physio) Mahatma Gandhi medical college and research institute , puducherry – India
HOPE THIS WOULD BE A VERY USEFUL LECTURE OR ATLEAST IT WILL BE A ---------FUL LECTURE
ANAESTHETISTS DO PREANAESTHETIC CHECK UP What is important ??
LAVOISIER AND LAPLACE 1779 • INTAKE OF SOME GASES WAS RESPIRATION AND IT PRODUCED SOME ACID • OXY= ACID • GENE= PRODUCER.
ATMOSPHERIC AIR • NITROGEN = 78% • OXYGEN = 21% • ARGON = 0.9% • CO 2 = 0.03% • TRACES OF HELIUM ,NEON AND KRYPTON
BAROMETRIC PRESSURE PB= 760 mm Hg • 760 × 21/100 =160 mm Hg. (PB × Fio2) HUMIDIFIED IN THE AIRWAYS. P H2O = 47 mmHg. PIO2 = (760-47) × 21/100 = 150 mmHg.
ALVEOLUS -- CO2 DILUTES PA02 = PIO2 – PACO2 / RQ = 150 - 45 = 105 RQ = RESPIRATORY QUOTIENT CO2 PRODUCED / O2 CONSUMED
ALVEOLUS ↓ O2 PLASMA ↓ O2 DISSOLVED OXYGEN ↓ TRANSFERRED TO Hb Pa O2 100 mm Hg
160 -150-105-100- 40-25-4 • oxygen cascade
OXYGEN CARRIAGE IN TWO FORMS • DISSOLVED — 0.3 ml / 100ml • Very less but., • IT IS IMPORTANT • IT DETERMINES PaO2 • IT TRANSFERS O2 TO HAEMOGLOBIN. • IT IS THIS SMALL QUANTITY WHICH DIFFUSES TO TISSUES FIRST.
HEMOGLOBIN • 1 gm of Hb carries 1.34 ml-1.39 ml of O2 • 19.5-19.7 ml oxygen / 100 ml • Dissolved + Hb oxygen= 20 ml • 200 ml / litre or 1000 ml / 5 litre
1000 ml o2 supplied • 250 ml consumed • 750 ml returned • SvO2 75% • Oxygen flux = CARDIAC OUTPUT × 1.34 × Hb × SATURATION
HEMOGLOBIN= HEME+GLOBIN • FOUR HEME MOLECULES +GLOBIN (FOUR CHAINS ) • 2 ALPHA AND 2 BETA CHAINS. • FOUR HEMES (FERROPROTOPORPHYRIN ) CAN ATTACH 4 OXYGEN MOLECULES • O2 + FERROUS = FERRIC → SATURATION → OXYGENATED Hb
COOPERATIVE EFFECT. • OXYGEN ENTRY TO Hb PROMOTES FURTHER ENTRY BY INCREASING THE AFFINITY UPTO 500 TIMES TO SUCK MORE O2----POSITIVE COOPERATIVE EFFECT. • IN DOWNLOADING IN TISSUES. REVERSE IS NEGATIVE COOPERATIVE EFFECT
Parrots and parents • Hemoglobin and oxygen act a little like parents and children. When all are living at home (i.e. hemoglobin is fully saturated) then the parents don’t want any to leave: • but once one has flown the nest (i.e. dissociated from hemoglobin) – parents find it progressively easier to let go.
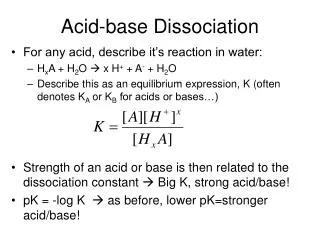
What this means that the conformation of the hemoglobin molecule depends on the number of molecules bound: • as one molecule of oxygen becomes unbound, the affinity for the others falls [and vice-versa]. • This is represented by the oxyhemoglobin dissociation curve.
Why the curve is sigmoid ?? • COOPERATIVE EFFECT CAUSES THE CURVE TO BE SIGMOID. • R FORM (RELAXED) –OXYGENATED • T FORM (TAUT) - DE OXYGENATED
BEFORE THE CURVE – A BREAK • A LADY PATIENT ENTERED A DOCTOR’S (MALE) CABIN AND SAID • “ SIR, CAN I ASK MY HUSBAND ALSO TO COME INSIDE.” • DOCTOR : “ BELIEVE ME, I AM A GENTLEMAN.”
LADY PATIENT : “SIR I BELIEVE YOU ., BUT I DON’T BELIEVE MY HUSBAND AND YOUR NURSE OUTSIDE”
SHIFT TO RIGHT = P50 > 27 • SHIFT TO LEFT= P50 < 27 • RIGHT SHIFT AT ANY PaO2 LESS AFFINITY ,LESS SATURATION • INCREASED H + IONS (ACID) • INCREASED PCO2, • INCREASED TEMP • INCREASED 2-3 DPG
BOHR EFFECT • ↑ PCO2 AND ACIDOSIS CAUSE RT. SHIFT • H + IONS BIND TO GLOBIN CHAINS TO EFFECT A CONFORMATIONAL CHANGE IN HEME ATTACHMENT FAVOURING UNLOADING OF O2 ( WE WANT TO HAPPEN IN TISSUES.)
HALDANE EFFECT • DEOXYGENATED BLOOD CAN PICK UP MORE CO2 • THINK OF TISSUES : • UNLOADING O2→ DEOXYGENATED BLOOD → PICKS UP MORE CO2
15 DAYS OLD BLOOD CAN CAUSE DECREASED 2-3 DPG LEVELS TO SHIFT LEFT--LESS UNLOADING AND MORE AFFINITY (KENNEDY EFFECT) • 24-48 HOURS TO BECOME NORMAL.
What is the role of 2-3 DPG ?? • In the deoxygenated T conformer, a cavity capable of binding 2,3-BPG forms in the center of the molecule. 2,3-BPG can occupy this cavity stabilizing the T state. Conversely, when 2,3-BPG is not available, or not bound in the central cavity, Hb can be converted to HbO2 more readily.
Useful increase in 2-3 BPG • HIGH ALTITUDE. • COPD • CYANOTIC HEART DISEASE • SEVERE ANEMIAS.
Fetal Hb (higher affinity) • Umbilical venous blood (20-25 mmHg O2) • DOUBLE BOHR EFFECT • Transfer of acids from fetal blood to maternal intervillous spaces—maternal Hb more acidic Rt shift—more unloading to fetus…fetal alkalosis shift to left-Hb F more affinity-more loading
MYOGLOBIN (HIGHER AFFINITY) • HYPERBOLIC CURVE –NO COOPERATIVE EFFECT. • IF MYO REPLACES ADULT Hb IT NEEDS DOUBLE THE AMOUNT AND WE WILL BE 12 POUNDS HEAVIER. • BUT THERE(IN MUSCLE) WE NEED A STORAGE SPECIALIST AS ADULT Hb IS TRANSPORT SPECIALIST.
OXYGEN FLUX = CARDIAC OUTPUT ×O2 CONTENT ---(MAINLY 1.34 × Hb × SATURATION ) • IN A PERIOPERATIVE OR A CRITICAL CARE SETTING MAXIMISE O2 DELIVERY BY MAXIMISING- • 1.CARDIAC OUTPUT. • 2.Hb. • 3.SATURATION.
HOPE THIS WOULD BE A VERY USEFUL LECTURE OR ATLEAST A COLOURFULONE