Download
1 / 24
240 likes | 263 Views
Learn about Mycobacteria, their slow growth rate and unique characteristics, such as acid-fastness and waxy envelope. Explore methods for identification, culture, and growth, as well as the pathogenesis, pathology, and treatment of Tubercle bacilli. Gain insights into primary infection, reactivation, tuberculin tests, and diagnostic laboratory tests. Understand the epidemiology, prevention, and control measures against Mycobacterial infections.

E N D
Mycobacterium, Chlamydiae, Rickettsiae 20 Rabiulawal 1430H/ 17 Mac 2009
Mycobacteria • Rod-shaped, aerobic bacteria, non-sporing, slow growth rate than most bacteria. • They do not readily stain, but capable of resisting decolourisation by acid or alcohol, hence “acid-fast” bacilli. • Acid-fastness depends on the waxy envelope. • Ziehl-Neelsen technique. • Mycobacterium tuberculosis, Mycobacterium leprae, Mycobacterium avium-intracellulare.
An acid fast stain is used to diagnose the presence of mycobacteria in tissue and cytologic preparations. Note the thin red rod-like organisms.
Identification • Culture: selective and non-selective medium. • A) Semisynthetic agar media - contain albumin, neutralises the toxic and inhibitory effects of fatty acids in the specimen. Use to observe colony morphology. • B) Inspissated egg media – plus Malachite green to inhibit other bacteria. • C) Broth media – small inocula, adding Tweens wet the media surface and permit dispersed growth of Mycobacterium. • Grow in clumps or masses because of the hydrophobic character of the cell surface.
Growth of Mycobacterium • Hydrophobic cell surface causes them to clump and inhibits permeability of nutrients into the cell.
Tubercle bacilli • Tubercle bacilli are resistant to drying and survive for long periods in dried sputum. • Mycobacterial cell walls can induce delayed hypersensitivity and some resistance to infection and can replace whole mycobacterial cells in Freund’s adjuvant. • A) Cell walls – rich in lipids, which largely bound to proteins and polysaccharides. Attribute for granuloma formation, caseous necrosis and acid-fastness.
On closer inspection, caseous necrotic tissue is seen to constitute the granulomas in this gross appearance of a Ghon complex. Most patients with primary tuberculosis are asymptomatic, and the granulomas resolve.
Tubercle bacilli • B) Proteins – when proteins bound to a wax fraction, they elicit the tuberculin reaction (sensitivity); can stimulate antibodies production. • C) Polysaccharides – role are uncertain.
Pathogenesis & Pathology • Proliferation of virulent organisms + interaction with the host = disease • 2 host responses: • 1) delayed-type hypersensitivity reaction to mycobacterial proteins. • 2) Cell-mediated immunity (CMI) activates macrophages to destroy mycobacteria-contained within their cytoplasm. • Tubercle bacilli spread by lymphatic channels and bloodstream. • Mycobacteria reside intracellularly in monocytes, reticuloendothelial cells, and giant cells.
Primary Infection & Reactivation • When a host has first contact with tubercle bacilli, acute exudative lesions develop. The lymph nodes undergoes massive caseation, which usually calcifies. • Reactivation is usually caused by tubercle bacilli that have survived in the primary lesion. Characterised by chronic tissue lesions, formation of tubercles, caseation and fibrosis.
The caseous necrosis is extensive, and cavitation is prominent. Such patients can be highly infectious.
Extensive cavitation of multiple granulomas of lung are typical for secondary tuberculosis from reactivation of primary infection or reinfection as an adult. Such lesions have a predilection for appearance in the upper lobes of the lung.
Tuberculin Test • Material is reactive tuberculoproteins. • Dose of tuberculin – a large amount injected intracutaneously into a hypersensitive host may give rise to severe local reactions and a flare-up of inflammation and necrosis at the main sites of infection, normally 5 TU (TU=tuberculin units). • Reactions – had primary infection with tubercle bacilli develops induration.
Diagnostic Laboratory Tests • 1) Specimens • 2) Decontamination and concentration of specimens – liquefy with N-acetyl-L-cysteine, decontaminate with NaOH. • 3) Smears - __________, __________tested for acid-fast bacilli by ________________; fluorescence microscopy with auramine-rhodamine stain. • 4) Culture : selective/non-selective; anticoagulated blood for M. avium complex; growth rate; pigmentation in the dark. • 5) DNA detection, serology, and antigen detection.
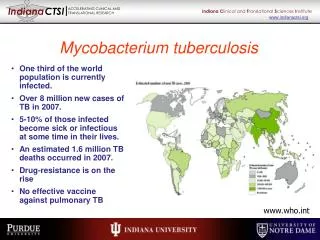
Treatment • Chemotherapy. • Tubercle bacilli prone to spontaneous mutants resistant to first-line antituberculosis drugs. • Rx: Isoniazid and rifampin. • Drug resistance to M tuberculosis is a worldwide problem.
Epidemiology • Source: human who excretes large number of tubercle bacilli, particularly from resp T; and close contact. • The development of clinical disease after infection may have a genetic component; age; undernutrition and by immunologic status; coexisting diseases (silicosis, diabetes, AIDS or HIV-infected patients).
Prevention & Control • 1) Prompt treatment, follow-up with tuberculin tests, x-rays. • 2) Drug treatment for asymptomatic tuberculin + persons. • 3) Reduced individual host resistance by starvation, gastrectomy, HIV-infected. • 4) Immunisation : BCG (bacillus Calmette-Guèrin, a live attenuated bovine organism@tubercle bacilli). • 5) The eradication of tuberculosis in cattle and the pasteurisation of milk have greatly reduced M. bovis infections.
Other Mycobacteria • Tubercle bacilli include M. tuberculosis, M. bovis. • M. avium complex commonly cause opportunistic infection ni AIDS. • M. kansaii is a photochromogen, can produce pulmonary and systemic disease identical to tuberculosis, esp in patients with impaired immune response.
Mycobacterium Leprae • Causes leprosy. • Are regularly found in skin scrapings or mucous membranes (nasal septum) in lepromatous leprosy. • Disease is divided into 2 types: lepromatous and tuberculoid. • Systemic manifestations of anemia and lymphadenopathy may also occur. Amyloidosis may develop.
Treatment and Prevention • First-line therapy is sulfones for both tuberculoid and lepromatous leprosy. • Leprosy is most likely to occur when small children are exposed for prolonged periods to heavy shedders for bacilli. Incubation period is probably 2-10 years. • Prevention is by identification and treatment of patients with leprosy, given chemoprophylactic drugs until the treatment has made them noninfectious.
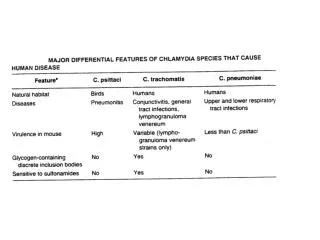
Chlamydiae • 3 species that infect human • Obligate intracellular parasites • All members of Chlamydiae exhibit similar morphologic features, share common group antigen, and multiply in cytoplasm by distinctive developmental cycle.
Cell pathology: • Elementary body EB • Reticulate body RB • (larger, devoid of electron-dense nucleoid) • 3. Cytoplasmic inclusion
Rickettsiae • Obligate intracellular parasites, are transmitted to humans by anthropods. • Staining: Giemsa, Gimenez, acridine orange. • Characterised by fever, headache, malaise, prostration, skin rash and enlargement of spleen and liver. These are the features of typhus fever. • Spotted fever and Q fever (resembles influenza, hepatitis, nonbacterial pneumonia). • Rx: tetracyclines, chloramphenicol.