Download

1 / 21
210 likes | 429 Views
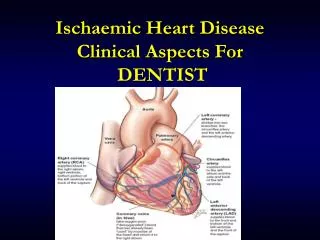
. Ischaemic Heart Disease. Etilogy. Most ischaemic heart disease is caused by atherosclerosis of the coronary artereries. Initially there is sudden sever narrowing or closure of large coronary arteries and or narrowing of coronary artery end branches. Covering plaques. Risk Factors. 1- age.

E N D
. Ischaemic Heart Disease dr.mon5@hotmail.com
Etilogy • Most ischaemic heart disease is caused by atherosclerosis of the coronary artereries. • Initially there is sudden sever narrowing or closure of large coronary arteries and\ or narrowing of coronary artery end branches. • Covering plaques......... dr.mon5@hotmail.com
Risk Factors 1- age. 2- Gender. 3- Serum cholesterol: VLDL....LDL...HDL. 4- Hypertension; endothelial damage. 5- Cigarate smoking; nicotine-----catecholamine-----epinephrine-----endothelial damage----lipolysis. 6- Diabetes; disturbed lipid metabolism. dr.mon5@hotmail.com
Minor risk factors 1- Hypothyrodism. 2- obesity. 3- Sedentary life. 4-Intellectual professional. 5- Contraceptive pills. dr.mon5@hotmail.com
Clinical Consequences A- Angina Pectoris Def. Clinical syndrome characterized by attack of pain due to ischaemia of the heart muscle, generally due to obstruction or spasm of coronary arteries. dr.mon5@hotmail.com
Types 1- Stable: occurs under similar circumstances, and with similar frequency over time. 2- Un-stable: • Recent onset. • Increased severity and frequency . • Angina at rest or with minimal exertion. 3- Variant: - At rest. - Spasm of coronary artery. -Not precipitated by increase myocardial 02 demand dr.mon5@hotmail.com
Clinical Picture • Pain: • Site • Radiation. • Character: burning..suffocation. stop all activities. - Precipitation: • Relief. • Duration. dr.mon5@hotmail.com
Associated Symptoms: Dyspnea . Palpitation. Dizzness. Fainting.Sweating. dr.mon5@hotmail.com
Clinical Picture: • Sings and symptoms: Pallor...tachycardia....hypertension. Investigation: • ECG: normal in 50%. • Stress ECG: Depression of st segment. Ventricular Arrhythmias. - Cardiac Catheterization : arteriography. - Echocardiography: regional wall abnor. Ex and rest. dr.mon5@hotmail.com
Therapy Aiming for : • Decrease myocardial oxygen demand. • Increase myocardial o2 supply. I. Medical Treatment: • Nitrates. Vosodilat.... Myo.02 sup • overload.... Myo o2 deman • Beta bolckers: • Calcium channel blockers • Antiplatelets: reduce incidence of MI dr.mon5@hotmail.com
II. Surgery: III. Preventive: 1- Avoid precipitating factors. 2- Control Risk factors. N.B . During Attack dr.mon5@hotmail.com
Myocardial Infarction Def. It is a medical condition that occurs when the blood supply to the heart is interrupted , and the myocardium is deprived of its blood supply ‘” therefore oxygen “’ for a significant amount of time. Pathogenesis: - Formation of occlusive thrombus at the site of rupture or erosion of atherosclerotic plaques in coronary artery. dr.mon5@hotmail.com
Clinical Picture: • Symptoms: • Prolonged cardiac pain: • Anxiety • Nausea . Vomiting • Breathlessness. • Syncope: Silent MI......elder....arrythmias dr.mon5@hotmail.com
II.Signs: • Signs of sympathatic activities: pallor, sweating, tachycardia • Signs of vagal activation: vomiting...bradycardia. • Signs of impaired myocardial function: hypotension. Narrow pulse pressure. - Signs of tissue damage. fever dr.mon5@hotmail.com
Investigation • ECG:- • Early • Late: • Advanced : 2) Blood test: • Cardiac enzymes: Cardiospecific isoform of CK :CK- MB Troponin T and I dr.mon5@hotmail.com
ESR: 3) Chest x ray: Pulmonary oedema. Cardiac enlargement dr.mon5@hotmail.com
Therapy A- Immediate Therapy: - High flow oxygen. • Aspirin 300 mg. • ECG monitoring. B) Acute perfusion therapy: 1- Thrombolysis: Help restore coronary potency. Preserve ventricular function. Improve survival. dr.mon5@hotmail.com
2) Primary percutaneous coronary intervension: C) Adjunctive Therapy: • Beta blockers relief pain ------reduce arrythmias. - Nitrates: Nitroglycerin: dr.mon5@hotmail.com