Download
1 / 24
240 likes | 585 Views
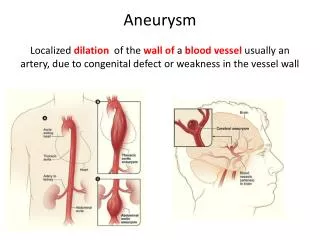
ISCHAEMIC HEART DISEASE Pathophysiology And Stable Angina Pectoris. JD Marx Department of Cardiology University of the Free State. Definition. The blood supply to the myocardium is insufficient to comply fully with physiological needs of the heart muscle. Pathophysiology.

E N D
ISCHAEMIC HEART DISEASEPathophysiologyAnd Stable Angina Pectoris JD Marx Department of Cardiology University of the Free State
Definition The blood supply to the myocardium is insufficient to comply fully with physiological needs of the heart muscle.
Pathophysiology • Blood supply - epicardial vessels with perforating branches • Blood flow from epicardium to endocardium
Pathophysiology • Control of blood flow • Perfusion in diastoly • Oxygen extraction maximal O2 supply can only be increased by increasing bloodflow • Humeral factors important - ADENOSIN
Pathophysiology • Factors influencing myocardial oxygen supply and demand Oxygen demand Oxygen supply Coronary bloodflow Duration of diastoly Coronary perfusion pressure Coronary vasomotor tone Oxygenation Haemoglobin Oxygen saturation • Heart rate • Blood pressure • Myocardial contractility
Auto-regulation Metabolic control Extravascular compressive forces Vascular resistance Diastolic phase Humoral factors Heart Rate Contractility Neural control Coronary blood flow Systolic wall tension O2-Carrying Capacity SUPPLY DEMAND
Pathogenesis Causes of vessel obstruction • Fixed lesions • Atherosclerosis • Arteritis • Embolization • Dynamic narrowings • Spasm
Pathogenesis Atherosclerosisis by far the most common cause of obstruction in patients with IHD
Pathogenesis Birth of Plaque
Pathogenesis Plaque progression
Pathogenesis Plaque rupture
Pathogenesis • Risk factors for Atherosclerosis Fixed factors Modifiable factors Smoking Hypertension Hypercholesterolemia Diabetes Mellitus Obesity Inactivity Stress • Family history • Gender - male • Age
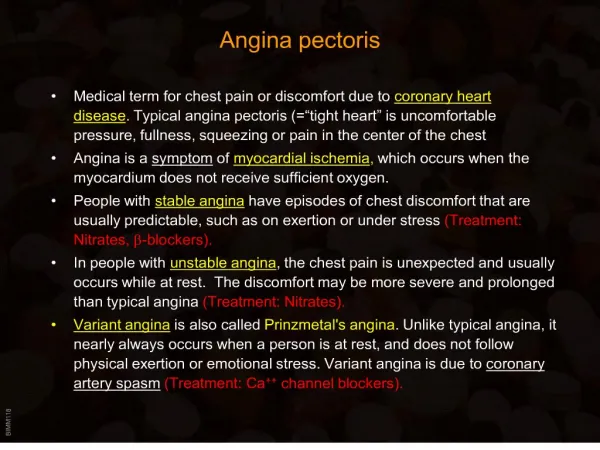
Clinical Presentation • of patients with Ischaemic Heart Disease • Stable angina pectoris • Acute Coronary Syndromes • Unstable Angina Pectoris • Non ST-segment elevation myocardial infarction • ST-segment elevation myocardial infarction • Arrhythmias • Sudden death • IschaemicCardiomyopathy with LV failure
Symptomatic Presentation • of patients with Ischaemic Heart Disease The patients most often present with chest pain which should clinically evaluated!
Symptomatic Presentation • Chest Pain ANGINA PECTORIS Typical chest pain caused by ischaemic myocardium
Symptomatic Presentation • Chest Pain Clinically patients with angina pectoris present with: • Stable Angina Pectoris • Acute Coronary Syndromes
Symptomatic Presentation • Chest Pain Chest pain resulting from a specific other disease process • Pericarditis • Pleuritis • Radicular or neural pain • Musculoskeletal pain • Gastroinstestinal pain • Other
Symptomatic Presentation • Chest Pain Atypical chest pain • The chest pain is not typical of any clinical disease entity • Several special tests necessary to evaluate
Angina Pectoris STABLE ANGINA PECTORIS • Diagnosis: • Clinical diagnosis: emphasis on history • Angina with stable pain pattern • Confirmed by: • Resting ECG • Stress ECG • Isotope perfusion study • Coronary angiography
Angina Pectoris Exercise Stress Test
Angina Pectoris Isotope Stress Test Exercise Rest
Angina Pectoris Angiogram LCA RCA
Angina Pectoris TREATMENT Conservative treatment: • General treatment • Aspirin • Anti-anginal medication • Nitrates • β-blockers • Calcium antagonists • Disease Modifying Therapy • Statins • ACE Inhibitors Interventional treatment: • Coronary angioplasty ( PTCA ) • Coronary Artery Bypass Graft Surgery ( CABG )