Download
1 / 25
270 likes | 539 Views
Risk assessment for VTE. Dr Roopen Arya King’s College Hospital. Prevention of VTE in hospitalised patients:. V. Documented mandatory risk assessment for all hospitalised patients. Why the need for risk assessment for VTE?. Identifying at-risk patient. Counselling at-risk patient.

E N D
Risk assessment for VTE Dr Roopen Arya King’s College Hospital
Prevention of VTE in hospitalised patients: V Documented mandatory risk assessment for all hospitalised patients
Why the need for risk assessment for VTE? Identifying at-risk patient Counselling at-risk patient Prescribe thromboprophylaxis
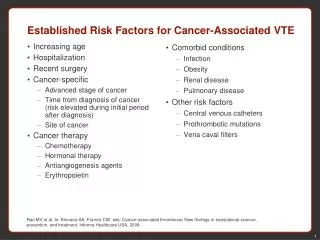
Risk Assessment • The highest ranking safety practice was the appropriate use of prophylaxis to prevent VTE in patients at risk. AHRQ “Making Health Safer: A Critical Analysis of Patient Safety Practices” 2001 • We recommend that every hospital develop a formal strategy that addresses the prevention of thromboembolic complications. This should generally be in the form of a written thromboprophylaxis policy especially for high risk groups. ACCP guidelines “ Prevention of VTE” 2004
Risk assessment models • Group-specific (‘opt-out’) • Individualized (‘opt-in’) • Risk stratification • Risk scores • Linked to ACTION of thromboprophylaxis
VTE risk assessment in surgical patients
Risk scoring for VTE: Kucher risk score Kucher, N. et al. N Engl J Med 2005;352:969-977
Primary end point: Freedom from VTE 100 98 Intervention 96 Freedom from DVT or PE (%) 94 P < 0.001 Control 92 90 Time (days) 0 30 60 90 Number at risk Intervention 1255 977 900 853 Control 1251 976 893 839 Kucher, N. et al. N Engl J Med 2005;352:969-977
Derivation and Validation of a Prediction Tool for Venous Thromboembolism (VTE):a VERITY Registry Study
Study objective • to develop a multiple regression model for VTE risk, based on Kucher, and validate its performance • to employ the extensive VTE risk factor data recorded in a UK VTE treatment registry (VERITY) • VERITY enrolls patients presenting to hospital with suspected VTE
UK multi-centre observational VTE registry of clinical management practices & patient outcomes
Features of VERITY • National registry – outpatient VTE treatment • Full spectrum of VTE – DVT and PE • Records information on patients presenting with suspected and confirmed VTE • Expanded data on demographics, presentation, management & outcomes • Extensive risk factor data
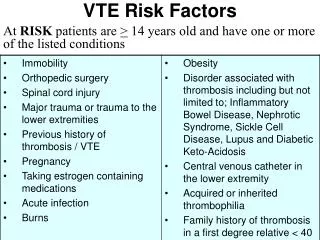
Statistical plan – model development • As a preliminary to a formal multiple regression analysis, the effects of the 8 Kucher risk factors on VTE risk were investigated individually by univariate analysis • Initial findings: univariate analysis (n=5928; 32.4% with diagnosis of VTE) suggested VTE risk was not accounted for by the 8 Kucher risk factors • An additional 3 risk factors were added (leg paralysis, smoking, IV drug use) and also patient sex, and the model was created with these 12 factors
Statistical plan – model development • The multiple logistic regression model was developed using backward stepwise regression • The open source statistical package ‘R’ was employed to conduct the regression analysis
Statistical plan – model performance • We tested the accuracy of the Kucher score and the new logistic regression model to classify patients by receiver operating characteristic (ROC) curve analysis, plotted as 1-specificity versus sensitivity for VTE diagnosis • The c statistic (area under the curve), representing the ability of the model to correctly classify patients, was estimated using the nonparametric method of Hanley and McNeil • We validated the model using a risk factor database of patients enrolled at an outpatient DVT clinic at King’s College Hospital
Statistical plan – model performance • We interpreted the predicted probabilities from the logistic regression model as a risk score • each tenth of predicted risk was scored as 1 • i.e. lower tenth of risk = risk score of 1; upper tenth of risk = risk score of 10 • We assessed the degree of agreement between the observed rate and the predicted rate of VTE by plotting the risk score vs. observed VTE rate • Differences in the rates of VTE vs. increasing risk score were assessed using the χ2 test for trend
Results - study populations VERITY n=55996 Assessment cohort (n=5938) 8 risk factors known VTE status known Univariate regression analysis Development cohort (n=5241) 12 risk factors known VTE status known Multiple regression analysis DVT O/P KCH n=928 Validation Cohort (n=915) 12 risk factors known VTE status known
Results – baseline characteristicsAssessment, development and validation cohorts
Results – risk factor findings in multiple logistic regression model
Pair-wise interactions for VTE risk in multiple logistic regression model
Receiver operating characteristic (ROC) curves for risk score prediction of VTE Kucher (––) c statistic 0.617 95% CI 0.599–0.634 VERITY (- - -) c statistic 0.720 95% CI 0.705–0.735 VERITY significantly better than Kucher (p<0.001)
Proportion of patients with VTE vs. risk score Strong positive correlation between an increasing risk score and the percentage of VTE-positive cases in the development cohort (P<0.001 by χ2 test for trend). VERITY risk score Kucher risk score
Validation cohort: ROC curves for risk score prediction of VTE Kucher (––) c statistic 0.587 95% CI 0.542–0.632 VERITY (- - -) c statistic 0.678 95% CI 0.635–0.721 VERITY c statistic no different from development cohort (p=NS)
Conclusions • The c statistic for this VERITY risk model (0.72) indicates a good test for likelihood of VTE diagnosis • This VERITY risk model was superior to Kucher for predicting the likelihood of a diagnosis of VTE in a cohort in whom the diagnosis was suspected • This risk model was validated in an independent VTE database • A prospective study is required to determine clinical value as a risk prediction tool for VTE at the time of hospital admission to assist in assessing prophylaxis needs