Download
1 / 44
480 likes | 835 Views
Risk Assessment for VTE. Which of the following best describes you?. Which of the following best describes your institution?. Do surgical patients in your hospital receive thromboprophylaxis?. Do medical patients receive thromboprophylaxis in your hospital?.

E N D
Do surgical patients in your hospital receive thromboprophylaxis?
Do medical patients receive thromboprophylaxis in your hospital?
Which of the following are used for thromboprophylaxis in your hospital?
Does your hospital provide extended-duration thromboprophylaxis?
Risk assessment for VTE • Risk • Risk assessment • Thromboprophylaxis risk assessment strategies
Risk assessment for VTE • Risk • Risk assessment • Thromboprophylaxis risk assessment strategies
What is risk? Risk can be defined as the probability of an unwanted event occurring and the severity of potential loss Risks exist because things considered to have value are placed at risk
Risk assessment for VTE • Risk • Risk assessment • Thromboprophylaxis risk assessment strategies
What is Risk Assessment? • Risk assessment consists of an objective evaluation of risk in which assumptions and uncertainties are clearly considered and presented. • Part of the difficulty of risk management is that the measurement of the quantities in which risk assessment is concerned - potential loss and probability of occurrence - can be very difficult to measure. Wikipedia
Risk Assessment for VTE • Potential losses: • Morbidity or mortality from VTE (including complications of therapy) • Financial cost of investigating and treating VTE • Increased future risk of VTE • Probability of occurrence: • Likelihood of patient developing VTE
Potential Losses from VTE • Morbidity • Post thrombotic syndrome in 30%, severe in 3-5%1 • Chronic thromboembolic pulmonary hypertension in 4-8% of patients following PE2 • Bleeding from anticoagulant therapies (1% major bleeding) • Mortality • 25,000 patients each year are thought to die of VTE in UK hospitals • Mortality from DVT 1-6% • Mortality from PE 10-30 • Mortality from anticoagulant therapies (0.3%/year) • Costs to healthcare system • Investigation and treatment of thrombotic episode • Prolongation of inpatient stay • Treatment of long term complications 1 Khan SR et al. Ann Int Med 2008 2 Dentali F et al. Thr Res Feb 2009
Probability of occurrence of VTE in hospitalised patients From ACCP Guidelines on prevention VTE Chest 2008
Most VTE cases are not detected 20% symptomatic 80% asymptomatic
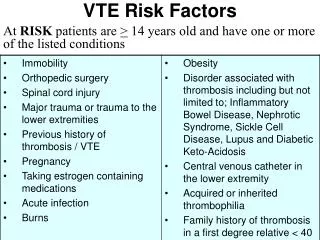
Risk Factors for VTE Patient characteristics Disease related Age Surgical therapy Trauma Obesity Cancer/ cancer therapies Varicose veins Cardiac/respiratory failure Immobility Myocardial infarction Pregnancy Paralysis of lower limb(s) Thrombophilia Infection Hormone therapy Inflammatory bowel disease Previous VTE Nephrotic syndrome Polycythaemia
Proportion of hospital inpatients at risk of VTE Endorse study Lancet 2008
Thromboprophylaxis strategies are required • It is, as yet, impossible to identify those individuals who will develop VTE • Screening using imaging techniques is of low sensitivity, expensive, time consuming • Asymptomatic DVT can cause fatal PE
Potential losses: risk of intervention • Adverse effects of prophylactic therapies • Bleeding • Dependent on surgical procedure • Intracerebral haemorrhage/ GI bleeding • Heparin Induced Thrombocytopenia • Dependent on prophylactic agent chosen • Higher with unfractionated heparin • Costs to healthcare system of adverse events
Risk assessment for VTE • Risk • Risk assessment • Thromboprophylaxis risk assessment strategies
Why Risk Assessment for VTE? Identify patients at significant risk of VTE Improve the use of appropriate thromboprophylaxis Objectives of RAM Simplify decision making Cost containment Reduce the burden of VTE Cohen AT et al.J Thromb Haemost 2003;1 (Suppl 1):OC437
Thromboprophylaxis Risk Assessment Strategies • Opt-in • Surgical only • Medical only • Hybrid models • Opt-out • Electronic risk assessment (opt in or opt out)
Opt-out model • Little evidence base • Advantages • Patients at risk of VTE possibly more likely to receive thromboprophylaxis • Disadvantages • Patients not at risk will receive prophylaxis • Patients are likely to be given prophylaxis even if at increased risk of side-effects
Information Technology helps Kucher, N. et al. N Engl J Med 2005;352:969-977
We recommend the use of strategies shown to increase thromboprophylaxis adherence, including the use of computer decision support systems, preprinted orders, and periodic audit and feedback. • Passive methods such as distribution of educational materials or educational meetings are not recommended as sole strategies to increase adherence to thromboprophylaxis Geerts et al, ACCP, Chest 2008
Risk assessment for VTE • Identify patients who would benefit from thromboprophylaxis • Strategy chosen will be dependent on • Culture of organisation • Local opinion • Information Technology • For strategy to work- needs to be simple
Rhona Maclean Sheffield Teaching Hospitals Consultant Haematologist Rhona.maclean@sth.nhs.uk