Download
1 / 73
820 likes | 1.58k Views
Nose and Paranasal Sinuses. Rabia Shihada Department of Otolaryngology – Head and Neck Surgery Bnai-Zion Medical Center. Anatomy: External nose. Bony: Nasal process maxilla Nasal bones Cartilages: Upper laterals Lower laterals Connective tissue Skin. Anatomy: Nasal cavities.

E N D
Nose and Paranasal Sinuses Rabia Shihada Department of Otolaryngology – Head and Neck Surgery Bnai-Zion Medical Center
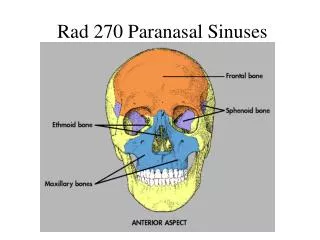
Anatomy: External nose • Bony: • Nasal process maxilla • Nasal bones • Cartilages: • Upper laterals • Lower laterals • Connective tissue • Skin
Anatomy: Nasal cavities • Lateral wall: • Turbinates(S/M/I) • Meati(S/M/I) • Sinus Ostia: • (esp MM) • Nasolacrimal duct (inf)
Anatomy: Nasal cavities • Floor: • =palate=roof of mouth • Roof: • =Ant. Cranial Fossa • Thin++ bone(Cribriform plate) • Dura & brain
Nasal cavities: Microanatomy: • Mucosal lining: • Respiratory epithelium: • columnar • goblet cells • mucus blanket • cilia • Olfactory epithelium: • Small area near roof
Vessels Involved • Anterior ethmoid • Posterior ethmoid • Greater palatine • Sphenopalatine • Superior labial Internal carotid External carotid
Epistaxis • Little’s area • An aggregation of poorly supported superficial vessels • Frequently the source of epistaxis
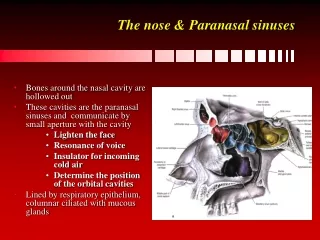
Paranasal sinuses: Anatomy: • Frontal • Maxillary • Ethmoidal • Sphenoid • “Outbuddings” from nasalcavity: continuous lining
Paranasal sinuses: Anatomy • Frontal • Close to: Brain, Eye • Thin walls esp: Brain, Eye • Maxillary • Ethmoidal • Sphenoid
Normal Sinus • Sinus health depends on: • Mucous secretion of normal viscosity, volume, and composition • Normal mucociliary flow to prevent mucous stasis and subsequent infection • Open sinus ostia to allow adequate drainage and aeration.
Development of Sinuses • Maxillary and ethmoid sinuses present at birth • Frontal sinus developed by age 5 or 6 • Sphenoid sinus last to develop, 8-10
Physiologic Importance of Sinuses • Provide mucus to upper airways • Lubrication • Vehicle for trapping viruses, bacteria, foreign material for removal • Give characteristics to voice • Lessen skull weight • Involved with olfaction
Symptoms Of Nasal Disease • Nasal obstruction • Nasal discharge • Pain • External deformities • Epistaxis
External Deformities Of Nose • Developmental: • deviation, narrowing • Trauma: • sinking of nose bridge due to haematoma or septalabcess • Diseases: • Syphilis, wegener, tuberculosis, cancer
Septal Deviation Of Nose • Origin: • developmental or traumatic • Symptoms: • nasal obstruction
Septal Deviation Of Nose • Treatment: • surgical: SMR or septoplasty • Complications: • alterations in nasal contour • perforation of septum
Nasal Polyps • Most common tumors of the nasal cavity • Associated with: • allergies • infection • trauma • metabolic disease • cystic fibrosis • asthma
Nasal Polyps Cont. • Symptoms include: • nasal obstruction • rhinorrhea • anosmia
Treatment Of Nasal Polyps • Surgical therapy: • polypectomy (with or without sinus surgery) • Medical therapy includes: • antibiotics • antihistamines • decongestants • desensitization • diet and steroids
Rhinitis or Coryza • “Common cold” • Mild, self limiting syndrome • Symptoms include: • nasal drainage and obstruction • sneezing • postnasal drip • sore throat • Symptoms last for 7-13 days
Rhinitis or CoryzaInfectious • Viral infection: • Rhinovirus 30-40% • Coronavirus 10% • Influenza >10% • Parainfluenza >5% • Adenovirus 5%
Rhinitis or CoryzaNon-Infectious • Allergic rhinitis: • IgE-mediated response causing release of vasoactive substances from mast cells.
Rhinitis or CoryzaNon-Infectious • Vasomotor rhinitis: • a nonspecific diagnosis of unexplained hypersensitivity.
Rhinitis or CoryzaNon-Infectious • Hormonal rhinitis: • Seen in pregnancy, at puberty and with the use of oral contraceptives. • Etiology: • increased estrogen levels • inhibited acytelcholinesterase • increased parasympathetic tone
Rhinitis or CoryzaNon-Infectious • Rhinitis medicamentosa • caused by excessive use of topical nasal decongestants.
Sinusitis • 4 paranasal sinuses, each lined with pseudostratified ciliated columnar epithelium and goblet cells • Frontal • Maxillary • Ethmoid • Sphenoid Infectious or noninfectious inflammation of 1 or more sinuses
Classification of Bacterial Sinusitis • Acute bacterial sinusitis- infection lasting 4 weeks, symptoms resolve completely (children 30 days) • Subacute bacterial sinusitis- infection lasting between 4 to 12 weeks, yet resolves completely (children 30-90 days) • Chronic sinusitis- symptoms lasting more than 12 weeks (children >90 days) • Some guidelines add treatment failure + a positive imaging study
Road to Bacterial Sinus Infections • Obstruction of the various ostia • Impairment in ciliary function • Increased viscosity of secretions • Impaired immunity • Mucus accumulates • Decrease in oxygenation in the sinuses • Bacterial overgrowth
Pathogenesis of Nasal Obstruction • Viral upper respiratory infections • Daycare centers • Allergic and nonallergic stimuli • Immunodeficiency disorders • Immunoglobulin deficiency (IgA, IgG) • Anatomic changes • Deviated septum, concha bullosa, polyps
Acute Bacterial Sinusitis • Usually begins with viral upper respiratory illness • Symptoms initially improve, but then … • Symptoms become persistent or severe • Persistent… 10-14 days but fewer than 4 weeks • Severe…temperature of 102°, purulent nasal discharge for 3-4 days, child appears ill • Disease clears with appropriate medical treatment
Bacteria Involved in Acute Bacterial Sinusitis 36 Streptococcus pneumoniae 30% Haemophilus influenza 20% Moraxella catarrhalis 20% Sterile 30%
Physical Findings • Mucopurulent nasal discharge • Highest positive predictive value • Swelling of nasal mucosa • Mild erythema • Facial pain (unusual in children) • Periorbital swelling
Treatment of Acute Sinusitis • Antihistamines recommended if allergy present • Oral or topical • Decongestants • Oral or topical • Antibiotic when indicated (bacteria) • Nasal irrigation • Hydration
When Medical Therapy for Acute Bacterial Sinusitis Fails… • Assess for chronic causes • Identify allergic and nonallergic triggers • Allergy testing, nasal smears for eosinophilia • Consider other medical conditions associated with sinusitis • Rhinolaryngoscopy • Imaging studies Sinus x-rays CT scanning (limited, coronal views)
Rhinoscopy Aids in Diagnosing • Nasal polyps • Septal deviation • Concha bullosa • Eustachian tube dysfunction • Causes of hoarseness • Adenoid hyperplasia • Tumors
MRI Imaging • Not used for imaging suspected acute sinusitis • Suspected fungal sinusitis • Suspected tumors
Chronic Sinusitis • Symptoms present longer than 8 weeks or 4/year in adults or 12 weeks or 6 episodes/year in children • Eosinophilic inflammation or chronic infection • Associated with positive CT scans • Poor (if any) response to antibiotics
Sx of Chronic Sinusitis • Nasal discharge • Nasal congestion • Headache • Facial pain or pressure • Olfactory disturbance • Fever and halitosis • Cough (worse when lying down)
Evaluation of Chronic Sinusitis • CT or MRI scanning • Anatomic defects, tumors, fungi • Allergy testing • Inhalants, fungi, foods • Sinus aspiration for cultures • Bacterial • Fungal • Immunoglobulins