Download
1 / 21
280 likes | 863 Views
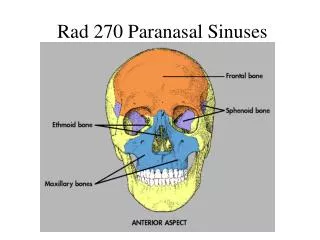
Paranasal Sinuses. Kristina Fatima Louise P. Garcia Group 5A1. Embryology of the Paranasal Sinuses. Develops as a diverticula of the lateral nasal wall Extends to the maxilla, ethmoid, frontal and sphenoid bones

E N D
Paranasal Sinuses Kristina Fatima Louise P. Garcia Group 5A1
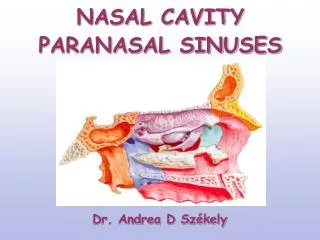
Embryology of the Paranasal Sinuses Develops as a diverticula of the lateral nasal wall Extends to the maxilla, ethmoid, frontal and sphenoid bones Reach maximum size at puberty and contribute to the definitive shape of the face The maxillary sinus is the only sinus routinely present at birth
Blood Supply:Paranasal Sinuses Conchae, Meatus and Septum sphenopalatine branch of the internal maxillary artery Ethmoidal and Frontal Sinuses and Roof of the Nose anterior and posterior ethmoidal branches of the ophthalmic artery
Blood Supply:Paranasal Sinuses Maxillary Sinus a branch of superior labial artery; infraorbital and alveolar branches of the internal maxillary artery Sphenoid Sinus pharyngeal branch of the internal maxillary artery
Nerve Supply • infraorbital nerve • posterior superior alveolar nerve • pterygopalatine ganglion (parasympathetic) • greater palatine nerve • lesser palatine nerve • cut nasopalatine nerve • nerve of the pharyngeal canal
All of the nerves are sensory branches of V2. • The pterygopalatine ganglion is suspended from V2 by two sensory roots. Since the ganglion is parasympathetic, there are preganglionic neurons feeding into it from the facial nerve (greater petrosal branch) that synapse at this point then continue onward as postganglionic neurons. • Their destination is the lacrimal nerve and reach there by rejoining the maxillary nerve through a sensory root, hopping onto the zygomatic nerve (V2), running up the lateral side of the orbit to jump onto the lacrimal nerve (V1) and then to the lacrimal gland to produce tears.
Physiology Olfaction Chemical Theory Undulation Theory Sinuses have no obvious physiologic function. Airway Resistance Variations in nasal resistance are due primarily to changes in the erectile tissues of the turbinates
Air Conditioning Inspired air is warmed (or cooled) to near body temperature and its relative humidity is brought to near 100 percent. Air Purification Hairs or vibrissae Solubility of gases Physiology
Mucociliary Function Transport of foreign particles is carried out via action of cilia moving the mucous blanket with its entrapped particles Pulmonary Correlations Speech Modification Physiology
Clinical Picture Signs and symptoms depend upon the sinuses involved Acute Sinusitis Maxillary = maxillary sinus and the adjacent midface and temple Ethmoid = over bridge of the nose and medial canthus of the eye Frontal = over the anterior wall and floor of the frontal sinus with pain radiating to the medial canthus Sphenoid = non-specific, marked by dull, aching pressure located at the center of the skull and radiating to the occiput
Diagnostics Rhinoscopy or nasal endoscopy Sinus radiograph Acute Sinusitis
Acute Sinusitis CT Scan MRI
Management Conservative: antibiotics, analgesics and decongestants Surgical: maxillary sinus puncture following decongestion and topical anesthesia of the nasal mucosa Sharp puncture, Blunt puncture, Beck puncture Acute Sinusitis
Chronic Sinusitis • Chronic inflammatory, allergic, traumatic, neoplastic • Impaired ventilation of the ostiomeatal unit due to stenosis and obstruction • Poor drainage > swollen mucosa esp at the narrow anatomical passages > recurrent bouts of inflammation > persistent, chronic sinusitis
Chronic Sinusitis • Diagnosis • Rhinoscopy, Endoscopy • Turbinate hyperplasia, pneumatized middle turbinate, concha bullosa, change in appearance of ostiomeatal unit, change in the nasal septum • CT Scan • Treatment • Decongestants, heat therapy, antibiotics, mucolytics • Sinus surgery – definitive treatment • Endoscopic sinus surgery
Mucoceles and Pyoceles • Mucocele – cystlike, mucus containing sac that can form within the paranasal sinus • Pyocele – mucocele containing purulent material (superinfection) • Caused by adhesions or mass lesions that obstruct drainage from the paranasal sinus system • Frontal > Ethmoid > Maxillary > Sphenoid • Obstruction > INC pressure on sinus wall > thinning of bone > erosion of mass
Mucoceles and Pyoceles • Clinical Picture • Frontal: isolated, tense swelling over the ant. wall of the frontal sinus, inferolateral displacement of orbital contents • Maxillary: swelling in the cheek area, upward displacement of orbital contents • Sphenoid: non-specific • Diagnostics • Prior surgical history, clinical appearance • CT, MRI • Treatment • Surgical removal