Download
1 / 150
1.57k likes | 1.91k Views
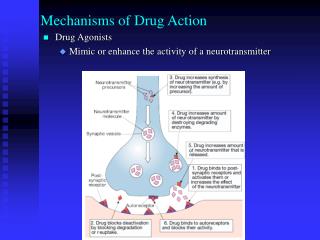
The Organic Chemistry of Drug Design and Drug Action. Chapter 5 Enzyme Inhibition and Inactivation. Enzyme Inhibition and Inactivation. Why inhibit an enzyme?. Many diseases arise from: deficiency or excess of one metabolite infestation of foreign organism aberrant cell growth.

E N D
The Organic Chemistry of Drug Design and Drug Action Chapter 5 Enzyme Inhibition and Inactivation
Enzyme Inhibition and Inactivation Why inhibit an enzyme? • Many diseases arise from: • deficiency or excess of one metabolite • infestation of foreign organism • aberrant cell growth All can be corrected by specific enzyme inhibition. Inhibition of an enzyme blocks the degradation of its substrate (increasing its concentration) and blocks the formation of its product (decreasing its concentration).
Enzyme inhibitor - slows or blocks enzyme catalysis Enzyme inactivator - irreversible inhibitor Use of drugs to combat foreign organisms and aberrant cells - chemotherapy About one-quarter of FDA-approved drugs are enzyme inhibitors Robertson, J. G. Biochemistry 2005, 44, 5561-5571.
Enzymes are the most promising protein targets for rational drug design because: • enzymes are purified more easily • enzyme inhibitors look like substrates • can use enzyme mechanism in design
Ideal inhibitor - totally specific for one target enzyme; rarely occurs, if at all • Look for differences in metabolic pathways between a foreign organism and humans • Look for substrate differences • Tumor cells have the same enzymes as normal cells, but replicate faster. They will take up antimetabolites (compounds that look like metabolites, but inhibit enzymes), which results in selective toxicity.
Ideal enzyme target in foreign organism or aberrant cell - one that is essential for growth, but nonessential in humans (or not even present)
Categories of Enzyme Inhibitors • Reversible - inhibition of enzyme activity that is reversible, typically noncovalent • Irreversible - inhibits enzyme for an extended period of time, typically covalent First, consider two important concerns in drug design: drug resistance and drug synergism.
Drug Resistance When a formerly effective drug dose is no longer effective. Arises mainly from natural selection - replication of a naturally resistant strain after the drug has killed all of the susceptible strains. On average, 1 in 10 million organisms in a colony has one or more mutations that makes it resistant.
Resistance is different from tolerance - this is when the body adapts to a particular drug and requires more of the drug to attain the same initial effect - lowers the therapeutic index. It is also possible to develop tolerance to undesirable effects of drugs, such as sedation by phenobarbitol - raises the therapeutic index.
Mechanisms of Drug Resistance 1. Altered drug uptake - exclusion of drug from site of action by blocking uptake of drug - altered membrane with more + or - charges 2. Overproduction of the target enzyme - gene expression 3. Altered target enzyme (mutation of amino acid residues at the active site) - drug binds poorly to altered form of the enzyme 4. Production of a drug-destroying enzyme - a new enzyme is formed that destroys the drug
Mechanisms of Drug Resistance (cont’d) 5. Deletion of a prodrug-activating enzyme - the enzyme needed to activate a prodrug is missing 6. Overproduction of the substrate for the target enzyme - blocks inhibitor binding 7. New metabolic pathway for formation of the product of the target enzyme - bypass effect of inhibiting the enzyme 8. Efflux pump - protein that transports molecules out of the cell
Examples of Mutated Target Enzyme M184V and M184I mutants are produced by HIV when exposed to these drugs If your drug has a structure similar to the substrate, mutations will lower binding of the substrate as well as the inhibitor.
Approaches When a Drug-Destroying Enzyme is Produced 1. Make an analog that binds poorly to this new enzyme 2. Alter structure of drug so it is not modified by the new enzyme, such as tobramycin (5.14), which lacks the OH group of kanamycins (5.12) that is phosphorylated by resistant organisms. no OH group resistant organisms phosphorylate here 3. Inhibit the new enzyme
Drug Synergism Arises when the therapeutic effect of two or more drugs used in combination is greater than the sum of the effect of the drugs individually.
Mechanisms of Drug Synergism 1. Inhibition of a drug-destroying enzyme protects the drug from destruction 2. Sequential blocking - inhibition of two or more consecutive steps in a metabolic pathway - overcoming difficulty of getting 100% enzyme inhibition 3. Inhibition of enzymes in different metabolic pathways- block both biosynthetic routes to the same metabolite 4. Efflux pump inhibitors can be made to prevent efflux of the drug 5. Use of multiple drugs for same target - about 1 in 107 bacteria resistant to a drug; if you use two drugs, then only 1 in 1014 is resistant to both
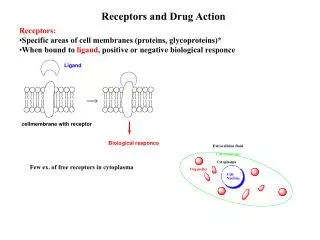
Reversible Enzyme Inhibitors Most common compete with substrate for active site binding - competitive reversible inhibitors; structures similar to substrates or products Scheme 5.3 (equilibrium attained with diffusion control) Dissociation constant for breakdown of EI complex The smaller the Ki, the tighter (more effective) the binding.
Inhibitor also may be a substrate - may be unfavorable in drug design if the product is toxic • Inhibitor can act by binding to a site other than active site (an allosteric site) - called a noncompetitive inhibitor • EI concentration depends on [I] and [S] and their dissociation constants (Kiand Km, respectively). As [I] increases, [EI] increases. • Both S and I compete for E, so as either [I] decreases (by metabolism) or [S] increases, [EI] decreases and [ES] increases. Therefore, drugs are administered several times a day to maintain the enzyme in EI complex.
Example of Simple Competitive Reversible Inhibition Captopril, enalapril, and lisinopril - antihypertensive drugs Scheme 5.4
Hypertensive Effects of ACE • Produces angiotensin II, a vasoconstrictor (hormone action) • Involved in conversion of angiotensin II to angiotensin III, which releases another hormone, aldosterone (5.23). This hormone regulates the electrolyte balance by retention of Na+ and water. • Catalyzes hydrolysis of a potent natural vasodilator, bradykinin Arg-Pro-Pro-Gly-Phe-Ser-Pro-Phe-Arg bradykinin
Lead Discovery • 1965 - mixture of peptides in the venom of a South American pit viper shows inhibition of bradykininase activity and inhibits conversion of angiotensin I to angiotensin II • 1971 - several other peptides found at Squibb but not effective orally • Today, a peptide combinatorial library approach would be taken.
Lead Modification Pro found best at C-terminal position, Ala best in penultimate position, and an aromatic residue in the antepenultimate position. ACE purified to homogeneity from rabbit lung - contains one Zn++/enzyme
Mechanism of Action Function of Zn++ cofactor Figure 5.5 May be similar to carboxypeptidase A, another Zn++-dependent peptidase.
Hypothetical Active Site of Carboxypeptidase A Figure 5.6 potent inhibitor of CPA
Potency of (R)-2-benzylsuccinic acid derived from its resemblance to the collected products of substrate hydrolysis. Figure 5.7
With (R)-2-benzylsuccinic acid as a model, a series of carboxyalkanoylproline derivatives were tested as inhibitors of ACE. good Zn++ coordination Peptidomimetic To avoid orally unstable dipeptide, made isostere All were only weak inhibitors of ACE.
Hypothetical Binding of Inhibitors to ACE Figure 5.8 isosteric exchange
Best binding properties Ki = 1.7 nM Highly selective for ACE
Effect of Structural Modifications Every part of captopril is important for binding. Table 5.1
Captopril was the first ACE inhibitor on the drug market - hypertension and congestive heart failure.
Combination Therapy diuretic (for water retention caused by aldosterone) • This combination is effective for 90% of the hypertensive population. • Sometimes a -blocker is used in triple therapy for vasodilation.
Two side effects: rashes and loss of taste - reversible when drug withdrawn • Merck hypothesized side effects from SH group. Went back to COO- instead of SH Increased potency by adding groups to interact with more sites on enzyme (i.e. - to increase the pharmacophore).
Made more peptide-like, but protonated; too hydrophilic Added a lipophilic group (R) to counteract hydrophilicity and also to bind to S1 subsite R = (S)-PhCH2CH2 R = H enalaprilat
Binding of Enalaprilat to ACE Figure 5.9 additional binding interactions enalaprilat Poorly absorbed orally - remedied by using ethyl ester (at arrow) (enalapril) which is hydrolyzed by esterases to give enalaprilat (a prodrug).
Dual-Acting DrugsDual-Acting Enzyme Inhibition When inhibition of two different enzymes gives a synergistic effect, a single inhibitor for both enzymes can be designed.
Advantages of making a dual-acting drug instead of two separate drugs: 1. With two drugs need to develop two separate syntheses, two formulations, and two metabolism studies. 2. Two drugs have different pharmacokinetic rates and metabolic profiles. 3. The likelihood that two drugs will progress to the clinic at the same rate is small. 4. Must do three sets of safety studies and three sets of clinical trials (one for each drug plus the combination). 5. The odds of one drug in clinical trials getting to market is 1 in 10; the odds of two drugs is 1 in 100.
Example of a Dual-Acting Enzyme Inhibitor • Neutral endopeptidase (NEP) is Zn++-dependent and degrades atrial natriuretic peptide (ANP). • ANP causes vasodilation (lowers blood pressure) and inhibits aldosterone formation. • Therefore, ANP and angiotensin II have opposite functions. • inhibition of NEP increases [ANP] • inhibition of ACE decreases [angiotensin II] • both result in blood pressure lowering
Peptidomimetic Dual-Acting Enzyme Inhibitors Bristol-Myers Squibb Lead modification Lead compound IC50 = 30 nMvs ACE IC50 = 400 nMvs NEP potent in vitro for both ACE and NEP poorly active in vitro
Conformationally-restricted Peptidomimetics potent in vitro and in vivo for both ACE and NEP IC50 = 5 nMvs ACE IC50 = 17 nMvs NEP oral activity greater than captopril in rats
The 7,6-fused bicyclic thiazepinone analogue was advanced to clinical trials: IC50 = 5 nMvs ACE IC50 = 8 nMvs NEP Problems in phase III clinical trials; had to be withdrawn.
Dual-acting drugs do not have to inhibit only enzymes. Could be an inhibitor of an enzyme and a receptor antagonist or an antagonist for two receptors, or an agonist for two receptors (or any combination thereof). • The approach is to identify molecules that interact with each receptor or enzyme, then combine parts of each molecule to identify what is a common pharmacophore.
Example of a Dual-Acting Receptor Agonist Agonist for both the D2-receptor and 2-adrenoceptor would be useful for the treatment of airway diseases, such as chronic obstructive pulmonary disease (COPD) and asthma.
D2-receptor agonist reduces cough and mucous • 2-adrenoceptor agonist is an antibronchoconstrictor a weak 2-adrenoceptor agonist a potent D2-receptor agonist These two were hybridized to give
Example of Competitive Reversible Inhibitor Drug that Also Acts as a Substrate Sulfonamide Antibacterial Agents (Sulfa Drugs) Lead discovery - Bayer Co. tested azo dyes against streptococci. Prontosil was very effective in mice (1935). prontosil No activity in vitro unless a reducing agent is added. In vivo protonsil is metabolized by reduction to the active agent (a prodrug).
sulfanilamide The active agent - active in vitro and in vivo Bacteriostatic - inhibits further growth of bacteria, but does not kill them.
Lead Modification • Prontosil - beginning of modern chemotherapy • Thousands of compounds synthesized and tested - the first SAR studies • First examples where new leads for other diseases revealed from side effects in clinical studies - antidiabetic and diuretic agents • Other developments from these studies: • a simple assay for these compounds in body fluids • showed antibacterial effect is proportional to the concentration in blood, which varied from patient to patient at a given dose - beginning of monitoring blood drug levels during chemotherapy
Mechanism of Action 1939 Stamp showed microorganisms contained a substance that blocked the antibacterial action of sulfonamides 1940Woods hypothesized that sulfanilamide must have a structure similar to a substrate for an essential enzyme He deduced that the structure was p-aminobenzoic acid (PABA) Showed that PABA was competitive with sulfanilamide for microbial growth