Download
1 / 57
570 likes | 697 Views
The World of HIV/AIDS. Photos (good ones) by Malcolm Linton. Overview*. History and Epidemiology Existing prevention strategies Existing treatment strategies Future treatment and prevention strategies * Heavily spiced with politics, economics, ethics, odd ideas and opinions. End of 2005,

E N D
The World of HIV/AIDS Photos (good ones) by Malcolm Linton
Overview* • History and Epidemiology • Existing prevention strategies • Existing treatment strategies • Future treatment and prevention strategies * Heavily spiced with politics, economics, ethics, odd ideas and opinions
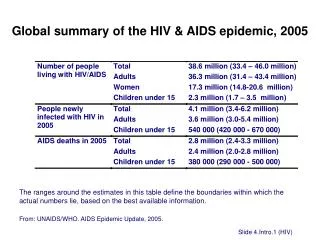
End of 2005, UNAIDS Total: 38.6M Sub-Saharan Africa: 24.5 M Asia: 8.3M LatAm and Carib: 1.9M 90% of infections in SSA, Asia, and LatAm and Carib
*First report in MMWR on June 5, 1981* 11 MMWRReports by September 1982
PREDICTIONS Blood test, widely available 6 months YES “We hope to have such a vaccine ready for testing in approximately two years,” HHS Secretary Margaret Heckler YES, BUT NO “What we have at the moment is not particularly of great benefit to people who have the disease…but it hopefully will be in a short while,” Asst. Sec. of Health, Edward Brandt NO The “Race” is On: April 23, 1984
The #1 Problem 9 subtypes If HIV were TB, a cure would exist If HIV were HBV or polio, a vaccine would exist today
Get Inside the Enemy’s Head HIV’s Profile Objectives: Copy and Spread Body Type: Retrovirus, RNA Attributes: No brains, morals or political agenda Desired residence: Anywhere Turn Ons: Anal Sex, Vaginal Sex, Injecting Drugs, Pregnancy Turn Offs: Condoms, ARVs, Clean needles, Immune System
We Aren’t the World • Countries, companies, research institutions have different agendas and needs • Organizing scientists is like herding cats • Politics continues to trump science
The Big Logistical Problems • Most HIV+ don’t know infected • Only 1.3 million of 5.5 million in need receive ARVs as of 12/05 • Scaling up treatment: monitoring, training, FDCs • Not much $ in vaccines, microbicides, generics • Prevention efforts woefully lacking
Sub-Saharan Africa has 10 countries with adult prevalence >10% Namibia: 19.6% South Africa: 18.8% Swaziland: 33.4% Zambia: 17.0 % Zimbabwe: 20.1% Botswana: 24.1% CAR: 10.7% Lesotho: 23.2% Malawi: 14.1% Mozambique: 16.1%
Why the high Prevalence in Sub-Saharan Africa? • Concurrent sexual partnerships both male and female • Intergenerational sex: Sugar daddies • Migration and poverty • Concurrent untreated STDs (HSV-2) • Lack of circumcision • Sex work and clients
Epidemiology: Gender differences Age and gender specific prevalence of HIV infection in rural South Africa 10 Male Female 8 JUN/JUL 92 6 Prevalence (%) 4 2 0 <9 10-14 15-19 20-24 25-29 30-39 40-49 Source : Abdool Karim Q et al, AIDS 1992
HSV-2 and Circumcision • 2 high prevalence cities, 2 low • ~1000 males and ~1000 females in each (Buve, AIDS, 2001)
Circumcising Adults? • Orange Farm, South Africa, August 2005
Asia • Huge populations in India and China: >1/3 of world • Injecting drug use: heroin producing • Sex work • Thai Success
India • Different epidemics • 5.7 million HIV+ • Adult prevalence: 0.9%
China • Blood plasma scandal • IDUs
Southeast Asia • Thailand: sex workers and IDUs • Myanmar/Burma: big heroin producer • Cambodia: No IDUs • Vietnam: IDUs
Preventing an IDU epidemic slows or averts a sex work epidemic…Projected epidemic in Jakarta with and w/o IDUs Pisani, FHI Indonesia
Doubling number of clients produces more rapidly growing epidemic By 2030, 13.2% of males, 5.4% of females HIV+ Brown/Wiwat, East-West Center
But prevention must be sustained.. If condom use falls, HIV rises, even in Thailand Supposing condom use drops to 60% starting 1998
Latin America and Caribbean • Caribbean: highest prevalence outside Sub-Saharan Africa • Latin America: Similar to Asia, but little IDU • Drivers: • Migration • Poverty • Sex tourism • Clients of sex work • MSM Contrasts Abound
Evolution of Epidemic • Starts in Haiti, 1982 cases surface
Haiti’s Successes • Lowered prevalence • Pioneered treatment of poor
Dominican Republic’s Challenges • Bateyes • Sex work • Treatment programs
Puerto Rico • IDU driven • Topnotch research • Topnotch care--for non-IDUs
Mexico and Central America • MSM • Migration • Wars, Gangs • Special populations • Sex Work
Garifunas Migration Regional wars MSM Sex workers Prisons Honduras Hotspot
Mexico • MSM • Anti-homophobia campaign • Migration
Guatemala:Treatment and Care Uneven • Centralized • Drug supply • Discrimination • Transition issues
South America • Brazil > ½ cases • Andean region MSM • Southern cone was IDU
Pioneered universal access Escalating costs Sex-positive prevention Brazil
Argentina • Epidemics change • Was IDU cocaine and MSM • Now primarily heterosexual
Peru • Research magnet • MSM • Leading researchers from community
Prevention Efforts Woefully Lacking • Scattershot targeting of high-risk groups • Treatment benefits prevention • 9 billion more condoms/year needed • Harm reduction for 3.6% of IDUs • ARVs for 3% of pregnant HIV+
Treatment Issues: Rich vs. Poor AZT d4T ddI ddC NVP EFV IND SQV 3TC FTC T-20 RT NRTI NNRTI PI FI CD4 CCR5 VL
The Cocktails Work Percentage of Patient-days on HAART Deaths per 100 Person-Years Frank Palella/HOPS
Other Treatment Limitations for Rich and Poor Countries Alike • Many HIV+ don’t know infected • Adherence: Simpler regimens needed • Training of clinicians • Proper monitoring • No cure exists
The Story of Henan Henan Province had 20% dropout first year, no 3TC, and NVP resistance in first 9 months was 20%-30%.
New Players $5.5 Billion Committed President’s Emergency Plan for AIDS Relief (PEPFAR) $15 billion/5 years $150 Million To Fund, >$500 Million to HIV Vaccine