Download
1 / 78
850 likes | 1.43k Views
Anatomy of thorax. Landmarks – anterior view. Supresternal notch Angle of Louis – cartilage of the 2 nd rib Xifoid apendix Subcostal angle Thoracic lateral wall Ribs 7, 8, 9, 10 Free ending 11, 12 Collar bone – acromion Projection of diaphragm (top ~ 5 th rib) Breast

E N D
Landmarks – anterior view • Supresternal notch • Angle of Louis – cartilage of the 2nd rib • Xifoid apendix • Subcostal angle • Thoracic lateral wall • Ribs 7, 8, 9, 10 • Free ending 11, 12 • Collar bone – acromion • Projection of diaphragm (top ~ 5th rib) • Breast • Anterior axilary line
Muscles of anterior thoracic wallsignificance in respiration
LandmarksPosterior view • Processus sipnosum • Scapula: • Superior angle – C2 • Inferior angle – C7 • Ridge • Muscular prominences • Latissimus dorsi • Trapesius • Erectori spinae
Lines used for orientatiom • Median • Midd-clavicular line • Axillary line • Anterior • Middle • Posterior • Scapulary line (through the inferior angle) – armes being close to the trunk
Superficial projections of respiratory aparatus • Tracheea: • Cricoid – angle of Louis • Lungs • C6-C8-C10 • Pleura • C8-C10-C12
Aortic arch, brchiocephalic trunk, inferior vena cava, brahiocephalic veins are projected behind the manubrium Internal thoracic vein – 1-3 cm lateral to the manubrium Intercostal vessels Heart projection Pericardium Superficial projection of the heart and great vessels
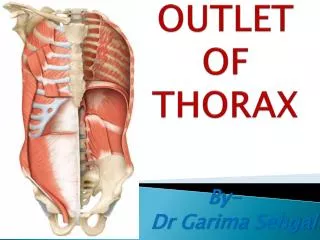
Communications of the thoracic cavity • Superior opening – base of the neck • T1 – C1 – manubrium • Tracheea, esofagus, great vessels from the neck • Inferior opening • T12 – costal margin xifoid apendix • Diafragm with openings ofering passage for • Esofagus, nerves vagus nerves • Aorta, inferior vena cava
Autoexamination of the breast • Begin after onset of hormonal sexual activity • Monthly – preferable after menstruation • Inspection • Volume, position, profile • Palpation
Medical examination of the breast • History taking • Borths • Breast feeding + duration • Menstrual activity + changes in the breast • Other lesions • Hormonal therapy • Palpation • Breast + breast tissue outside “gland” • Nipple • Axillary lymph nodes • Skin • COMPULSURY BOTH SIDES
Axillary lymphnodes • External thoracic (under the pectoralis major) • Main collector • Brahial group • Inferior scapullary group - dorsal • Subclavicular – top of axxila • Central • Internal thoracic – not accesible
Imagistics • Ultrasound scan • Doppler effect for vessels diposition • Mamography • Galactograpy
Pain Relatively minor element that triggers changes in ventilation Significant presence in any thoracic trauma Immobilization – not applicable Suppresses cough reflex Finally generates airway obstruction and hypoxia Pneumotorax Major deficit – loss of functional pulmonary tissue Complex mechanism Airway obstruction Acute respiratory failure fearful complication Tahipnea Acute dispneea Use of accessory respiratory muscles Cyanosis Anxiety Common manifestations in thoracic trauma
Non-characterisctic symptoms Ecchymosed Hematoma Subcutaneous fluid collections Muscle tears As a single lesion – children (soft thorax) Clinically – same as any other locations Contusions of soft tissue
Sternal fractures • Mechanism • Direct impact • Acute flexion • Type: • transversal w/o movement of fragments • Particular situation – manubrio-sternal disjunction • Clinically • Pain • Deformity • Short sternumt with dimished intercostal spaces
Costal fractures • Very frequent in adulthood – 10% • More frequently in ribs situated in the middle unprotected area • Direct or indirect mechanism • Direct – sharp bone projected inside • Indirect – sharp bone projected outside
Clinically Benign lesions Pain Diminished amplitude of respiratory movements Palpation – in the arrea of fracture Deformity Osseous creptiations during deep inspiration or cough MAJOR risk Lesion of pleura or lung Direct lesions Parietal pleura Visceral pleura Lungs Intercostal vessels Indirect lesion Intercostal vessels Costal fractures
Blood acumulation in the pleural space Vascular lesions in the intercostal space (intercostal artery – very important hemprrhage) Pulmonary lesions Mediastinal lesions Clasification Small: 300-500 ml occupies the costo-diafragmatic angle and has limited symptoms. Medium: <1500ml reaches the middle of the scapula Large: >3000 ml Hypoxia lung is compressed Circulatory changes – mediastinal shift Hypovolemia Hemothorax
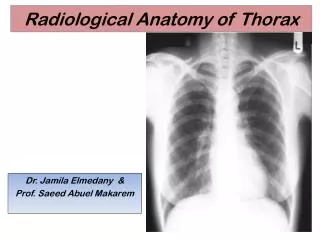
Hemothorax • Clinical examination • Dull on percution • Respiratory sounds not audible on the affected side • Diminished amplitude of respiratory movements • Chest X-Ray • Pleural puncture – will show the nature of the fluid (blood)
Typical hemothorax – secondary to rib fractures Massiv hemothorax Small – in decubit the fluid extends and shadows all the lung
Pneumothorax • Continuity between the lung and pleural space – during breathing in air gets in the pleural space • Aer tends to migrate: • Through the fracture area • Through pleural ruptures • Through natural communications of the chest (mediastinum, neck, etc)
Mechanism Pleural and pulmonary lesion Wound – aer coming from outside Calsification Small / medium /massiv Exmanition: Thoraci pain Acute sensation of thoracic constriction Diminished amplitude of respiratory movements. Tympanic sound on percution Diminished amplitude of transmitted respiratory sounds!!!! IT MAY BE TRANSMITTED FROM THE OTHER SIDE Enclose pneumothorax
Open pneumothorax • Open wound in the thoracic wall • Air freely enters and exits during expiration • Air does not accumulate and does not increase pressure inside pleural space
Tension pneumothorax • Wound in the parietal or visceral pleura • Air enters the cavity REPEATIDLY with each inspiratory movement • The wound spontaneously closes during expiratiosn • Accumulation of air in the pleural space • Internal or external one-way mechanism
Acute onset Hypoxia, Respiratory distress, Cyanosis Agitation Sensation of imminent death Mediastinal compression (in advanced stages) Diminishes the functionality of the “normal lung” Decreases heart diastolic filling (angulation of SVC and IVC) End point – Acute Respiratory Failure and Acute Circulatory Failure Urgent decompression Tension pneumothorax - symptoms
Complex thoracic fractures –at least 3 ribs each with 2 fractures Typical mechanism is by compression of thorax Associates complex iternal organ trauma = Multiple trauma patient Classification Ventral (including the sternum) – frequent in car accidents impact on the steering wheel Anterior and lateral Lateral Dorsal (unlikely – big muscular structures) Flail chest
Flail chest • According to mobility • Fix – at least temporarily • Mobil • Similar to fluid effusion • Part of thorax escapes the action of respiratory muscles • Thorax no longer rigid • PARDOXICAL MOVEMENT
Flail chest • Complex respiratory disfunction • Decreased pulmonary capacity • Swinging air • Mediastinal shift • ARF and ACF • Surgical emergency
Contusions of the rachis • Fracture-dislocation • Mechanism: rotation or hyperflexion • Pathology : dislocation of vertebra and spinal cord compression • Clinically: neurologic defect, hematoma, subcutaneous hemorrhage + unequal intervertebral spaces • Fracture of vertebral body • Mechanism: compression + flexion = vertebral surfaces not parallel • Clinically: pain, musculare contraction, dorsal deformity of the spine, usual without neurological signs
Other contusions • Pulmonary contusions • Diaphragmatic contusions with diaphragmatic hernia • Contusions of the heart and pericardium • Trachea and bronchi contusions • Esophageal contusions