Download
1 / 37
370 likes | 593 Views
Angioplasty Coding. ASDIN Coding University. Angioplasty Coding. Angioplasty may be venous or arterial; these have different codes and special rules that relate to each Additionally, an angioplasty may be done in the upper or lower extremity Venous angioplasty – the same principles in both

E N D
Angioplasty Coding ASDIN Coding University
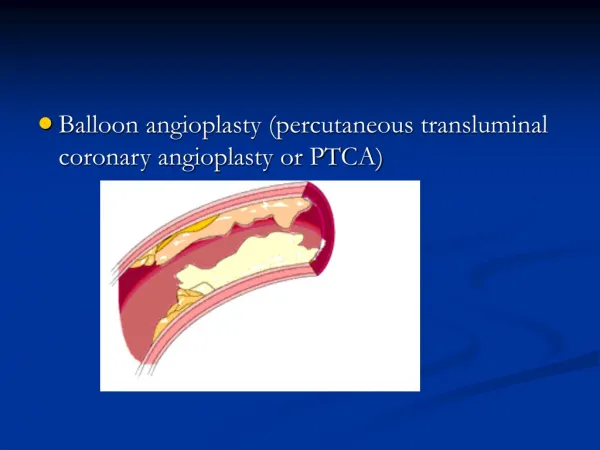
Angioplasty Coding • Angioplasty may be venous or arterial; these have different codes and special rules that relate to each • Additionally, an angioplasty may be done in the upper or lower extremity • Venous angioplasty – the same principles in both • Arterial angioplasty – in the lower extremity, the Lower Extremity Revascularization coding system is used (For arterial angioplasty in the lower extremity see separate unit)
Dialysis Access Definitions • Two different definitions: • For diagnostic purposes - the dialysis access is defined as beginning with the arterial anastomosis and extending to the right atrium • For therapeutic purposes - the dialysis access is defined as beginning with the arterial anastomosis and extending up to the beginning of the central veins • These apply to both an upper and lower extremity access
Venous System Definitions • For coding purposes the access is considered to be a separate vessel • Peripheral veins – the venous system up to the beginning of the central veins • Upper extremity – up to subclavian • Lower extremity – up to inguinal ligament (external iliac) • Central veins: • Upper extremity – veins within the boney thorax • Lower extremity – veins within the boney pelvis
Cannulation • Cannulation with angiogram – 36147 • The first cannulation of the access • Bundles the angiogram of the access (75791) • This includes all necessary angiographic imaging including the adjacent arterial inflow (approximately 2 cm), arterial anastomosis through the entire venous outflow including the inferior or superior vena cava (Refer to the separate unit on Cannulation/Catheterization for more detail on this subject)
Aids For Difficult Cannulation • In some instances the cannulation of the dialysis access is very difficult to accomplish, this is particularly true in the case of new or failing AVF • Two possible aids to assist this process are sometimes used; • Ultrasound guidance for the cannulation procedure • Using some type of device as a target
Ultrasound Guided Cannulation • Code for ultrasound guided cannulation is +76937 • An add-on code, use with cannulation code (36147) • Descriptor for this code is – ultrasound guidance for vascular access requiring ultrasound evaluation of potential access sites, documentation of selected vessel patency, concurrent realtime ultrasound visualization of vascular needle entry • Use of code requires image documentation in record
Device as Target • Angioplasty balloon or other device may be used • Generally done with fluoroscopic guidance • Code – 77002 - fluoroscopic guidance for needle placement • Column 2 code to 36147 • It can be used but requires a modifier (59 for example) • +77001 cannot be used in conjunction with 77002
Angiogram • This involves the access definition listed for diagnostic purposes (on slide 3) • May be performed in 2 ways: • With cannulation of access – bundled with 36147 (slide 6) • Without cannulation of access – a separate site, not part of the access as defined is used – coded as 75791 • Brachial artery (36120) or radial artery (36140) • Pre-existing cannulation site
Repeat Angiograms • Although an angiogram may be repeated several times during the course of the angioplasty procedure, it should be coded only once • Angiograms performed in follow-up for procedures such as angioplasty or stent placement are considered to be bundled with the basic procedure itself • Only exception is a follow-up angiogram following coil placement - code 75898 • It requires a 59 modifier since it is a therapeutic RS&I code and it is being used with a therapeutic RS&I code
Venous Angioplasty • Code is 35476 • Descriptor – transluminal balloon angioplasty, venous • This code should be used for an angioplasty anywhere within the entire venous system – venous portion of access and central veins • Used for both upper and lower extremities
Column I/Column II Restrictions • 35476 is a column 2 code when paired with 35475 (arterial angioplasty of the upper extremity) • The two can be used together, under specific conditions, but with a modifier attached to 35476 (59) • 35476 should be used only once in any case within the access, as defined for therapeutic procedures • 35476 cannot be used with 35475 except when a central vein is treated in addition to the arterial anastomotic lesion • If both an arterial and a venous angioplasty are performed within the access as defined for therapeutic purposes, only the arterial procedure (35475) should be recorded
Other Requirements • The degree of stenosis should be recorded in general terms (exact percentage may be difficult to define) • A stenosis of 50% as well as a clinical indication of dysfunction should be required prior to angioplasty
Accompanying RS&I Code • 35476 should always be coupled with its RS&I code 75978 • Descriptor for this code - transluminal balloon angioplasty, venous, radiological supervision and interpretation
Arterial Angioplasty • Two categories: • Upper extremity • Lower extremity • Coded differently
Arterial Angioplasty – Upper Extremity • Arterial angioplasty code – 35475 • Descriptor - transluminal balloon angioplasty, brachiocephalic trunk or branches, each vessel • Two situations exist: • Within the access as defined for therapeutic purposes • Arterial anastomosis • Within the artery proximal to the access as defined
Within the Access • The arterial portion of the access as defined is the arterial anastomosis • This is also taken to include approximately 2 cm of the adjacent artery • The artery proximal to this is not part of the access and its coding is governed by different principles
Juxta-Anastomotic Portion of Access • The juxta-anastomotic portion of the access is venous • When treating a juxta-anastomotic lesion, it is difficult to define radiographically exactly where the anastomosis (the arterial portion) is located • The guiding principle is - when the balloon must be in the artery in order to perform the angioplasty, it should be coded as an arterial angioplasty – (35475) • If this positioning is not necessary, then the juxta-anastomotic lesion should be coded as venous (35476)
Within the Access • 35475 is a column 1 code when paired with 35476 within the access as defined for therapeutic purposes • When both 35475 and 35476 are performed in this region only 35475 is recorded • If 35476 is performed within the central veins, both the 35475 and the 35476 can be recorded with a 59 modifier on the venous code
Within the Artery Proximal to the Access • Defined as artery more than approximately 2 cm from the arterial anastomosis • Not considered part of the access • Each lesion in a separate named artery can be individually coded as 35475 • Only one code should be used for each named artery • If an arterial lesion is continuous with a lesion at the anastomosis it should not be separately coded no matter how extensive it might be
RS&I Code For 35475 • For the first usage of 35475 the RS&I code is 75962 • Transluminal balloon angioplasty, peripheral artery other than renal, or other visceral artery, iliac or lower extremity, radiological supervision and interpretation • All subsequent usages of 35475 would require +75964 as the RS&I code • Transluminal balloon angioplasty, each additional peripheral artery other than renal, or other visceral artery, iliac or lower extremity, radiological supervision and interpretation
Arterial Angioplasty – Lower Extremity • Coding for an arterial angioplasty in the lower extremity requires the use of the Lower Extremity Revascularization coding system • See separate unit for a discussion of the application of this system to dialysis vascular access
Coding for Multiple Angioplasties • Situations in which multiple angioplasties may be coded are very limited • Most of the principles involved here have already been listed, but will be repeated for completeness • In applying these principles the definition of the access for therapeutic purposes is important • Includes the vessels from the arterial anastomosis up to the beginning of the central veins (subclavian)
Principles for Multiple Angioplasty Codes • Although multiple stenotic lesions may be present within the access as defined, their treatment only warrants only a single 35476 code • Although multiple stenotic lesions may be present within the central veins as defined, their treatment only warrants only a single 35476 code • If multiple stenotic lesions are present within the arteries proximal to the access, treatment(s) within each separate named artery can receive a separate 35475 code
More Multiple Code Principles • A 35476 code for a lesion within the access cannot be used with a 35475 code for a lesion at the arterial anastomosis • 35475 is a column 1 code, 35476 is a column 2 code • A 35476 code for a lesion within the access can be used with a 35475 code for a lesion in an artery proximal to the access • The 35476 code should have a 59 modifier attached
More Multiple Code Principles • A 35476 code for a lesion within the access can be used with a second 35476 code for a lesion within the central veins • The second 35476 code should have a 59 modifier attached • Only 2 angioplasty code (any type) can be used in a case related to the access • Anastomotic lesion + central venous lesion • Access venous lesion + central venous lesion
Events That Do Not Justify Multiple Codes • Performing multiple angioplasties from separate cannulation sites does not warrant multiple codes • If the access has a double drainage and both have lesions that are treated, it should be coded as a single angioplasty • If the case involves a bidirectional fistula and both limbs have lesions that are treated, it should be coded as a single angioplasty • The use of multiple balloon inflations or multiple balloon catheters is not enough to warrant multiple angioplasty codes
Second Cannulation • Each additional cannulation requires that the code +36148 should be used (1st is always 36147) • Not true if lower extremity arterial angioplasty is done • Descriptor - introduction of needle or catheter; arteriovenous shunt created for dialysis (graft/fistula) as an additional access for therapeutic intervention (See unit on Cannulation/Catheterization for more details on this code)
Arteriogram • An arteriogram is commonly done as a routine in most cases, but the code should not be recorded unless there is a clear medical indication • The code for an arteriogram is 75710 • Descriptor – angiogram, extremity, unilateral, radiological supervision and interpretation • If 75710 is applied in conjunction with a therapeutic RS&I code, it should have a 59 modifier attached • The technique used to perform the arteriogram does not affect the use of the code
Arteriogram Coding Principles • An examination of the artery adjacent to the arterial anastomosis is included in the 36147 code • This should be interpreted as being within approximately 2 cm of the anastomosis • Use of the 75710 code would be warranted only if you examined a larger segment of the artery • Examination of the entire artery is not required • The general rule should be – examine that portion of the artery that is necessary to make a diagnostic evaluation related to your medical indication
Medical Indications for Arteriogram • In general, there are two basic indicationsfor the performance of an arteriogram: • Evaluation of inflow in cases in which it is deemed to be inadequate for access function or where steal syndrome is suspected • Evaluation of the distal arterial run-off in cases suspected of having an arterial embolus
Hold True To Indication • What is done should hold true to the indication • Evaluation of inflow – should include an evaluation up to the aortic arch • Evaluation of distal run-off – should include an evaluation of the vessels distal to the bifurcation
Direct Cannulation of Artery • In some cases it is necessary to cannulate the artery directly • The code for cannulation of the brachial artery is 36120 • Descriptor - introduction of needle or intracatheter; retrograde brachial artery • The code for cannulation of the radial artery is 36140 • Descriptor - introduction of needle or intracatheter; retrograde extremity artery • In this instance the angiogram code 75791 would be used since 36147 has not been recorded (See unit on Cannulation/Catheterization for more details on these codes)
Complication Management CodesStent Placement See separate unit on Stenting for details
Important Note • This document is for informational purposes only and should serve as a guideline for appropriate coding. • The ultimate responsibility for correct coding /documentation remains with the provider of service. • ASDIN makes no representation, warranty, or guarantee that this compilation of information is error-free, nor that the use of this guide will prevent differences of opinion or disputes with CMS or any other carrier. • ASDIN will bear no responsibility or liability for the results or consequences that may grow out of the use of this guidance.