Download
1 / 21
260 likes | 409 Views
Join Dr. Stephen Hoole, an Interventional Cardiologist, at the 5th Annual Scientific Meeting on March 16, 2017, at the Museum of London to discuss the unmet needs in treating inoperable Chronic Thromboembolic Pulmonary Hypertension (CTEPH). Learn about the innovative BPA treatment algorithm, procedural details, possible complications, and our data in context.

E N D
Balloon pulmonary angioplasty Dr Stephen Hoole, Interventional Cardiologist 5th Annual Scientific Meeting Thursday 16th March 2017 Museum of London
Overview CTEPH unmet need for inoperable patients Treatment algorithm BPA Procedural details Our data in context Possible complications
CTEPH – an unmet need Chronic thromboembolic pulmonary hypertension (CTEPH) Persistent symptomatic pulmonary emboli at 1 year Prevalence: 8 - 40 cases per million population Mortality (untreated): 90% at 3-years Current treatments: Pulmonary endarterectomy (PEA) and medical therapy (pulmonary vasodilators, warfarin, LTOT) 40% CTEPH patients are inoperable
Treatment pathway • No impact on mortality • Expensive +++ • Improves • Haemodynamics • Morbidity and Mortality • Invasive +++ 60% 35% 5% Balloon Pulmonary Angioplasty
Procedure details Anticoagulation stopped 5 days before – transitioned to LMWH stopped night before RFV 7F Heparin 70u/kg BPA performed under conscious sedation (2hr procedure) Remifentanil (cough suppression) + midazolam Segmental 4mm balloon / sub-segmental 2mm balloon (balloon-to-artery ratio 0.5 – 0.8: 1.0) ROS after 2 hrs when ACT<175sec Bed rest 4 hrs
National BPA Service started on 2/10/15 Monthly BPA all-day list – treating 3 patients per list
A typical BPA case: RLL A8 Post Pre
Initial Post-operative care ITU/ HDU Monitoring: ECG and Saturation monitor Post procedure CXR Recommence LMWH and warfarin or NOAC alone on evening of procedure Transfer to chest medical unit post-op day 1-2 Monitor Saturations Creatinine Discharge home post-op day 3-4
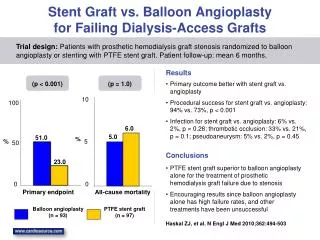
Our first 48 procedures… 16 patients treated with a median of 3 procedures each (range 1 – 6) Safety – 4 minor complications 3 access site haematomas 1 mild lung RI Efficacy – subjective symptomatic improvement and objective reduction in PVR* (-33.5%, p<0.001) and increase in 6 minute walk distance (+14.2%, p=0.05).
Reperfusion Oedema Segmental pulmonary oedema at day 0-7 due to lung suddenly exposed to high pulmonary pressure Prevention Treatment - supportive • Highest risk patients • 1st procedure • High PVR > 1000 dyn·s/cm5 • High mPAP > 35mmHg • Procedure staged in several sessions • 1-2 sub-segmental arteries • Smaller balloon size (0.5-0.8:1 ratio) • Limit the volume of lung exposed to high mPAP and endothelial shear force Optiflow Oxygen therapy CPAP IV Steroids? Prostacyclin?
Pulmonary artery perforation Presentation (in lab) Treatment cascade Balloon tamponade Gel foam via a pulmonary artery microcatheter Pulmonary artery coil Protamine Intubation and ventilation Transfuse if Hb<80g/L V-A ECMO Surgical repair Local contrast extravasation • Cough and haemoptysis • Hypoxaemia and shock
Right heart failure Presentation Treatment cascade Carefully consider fluid status Increase RV preload and EF vs. LV compression Titration of iv fluid/ diuretic carefully Good oxygenation Pulmonary vasodilator Inotropes Dobutamine Pulmonary vasodilators iNO/ iloprost/ ET-1 antagonists/ PDE-5 antagonists Further BPA? Atrial septostomy/ R-P Impella / ECMO or RVAD HLT • Hypotension • Hypo-perfusion/ Oliguria • Echo – RV dilatation, reversed IVC flow
Contrast Induced Nephropathy Presentation Treatment Prevention better than cure Minimise contrast dose Optimal hydration status Supportive Maintain fluid and electrolyte balance Severe cases may require renal replacement therapy • Definition: • Increase in Cr >25% or 44umol/L absolute increase at 72hrs
Funding for BPA Papworth Charitable funding for first 2 years Approximately £2-3,000 per case if no major complications requiring ICU Costs largely covered by pulmonary angio/ RHC tariff NICE appraisal on going National Commissioning decision awaited
The future… Increase capacity after funding approved Collect and publish data Develop BPA technique e.g. day case Understand intraoperative and post-op metrics of success e.g. RV function European BPA working group (1st BPA Meeting at European Heart House 13th October 2016). European Registry data and consensus statement on practice