Download
1 / 77
910 likes | 1.45k Views
Pituitary Adenomas : An Overview. Aashish Bhatt 9/29/2011. Anatomy of Pituitary. Location - Sella Turcica (Sphenoid bone in the middle cranial fossa) Weight - 60 mg Size – 1.5 x 1.2 cm Borders - Diaphragma sellae ( dural fold) Lateral sinuses Sphenoid sinuses

E N D
Pituitary Adenomas : An Overview Aashish Bhatt 9/29/2011
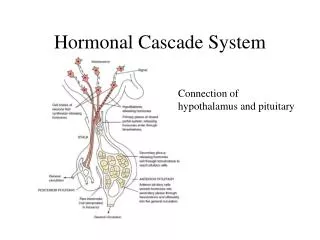
Anatomy of Pituitary • Location - SellaTurcica (Sphenoid bone in the middle cranial fossa) • Weight - 60 mg • Size – 1.5 x 1.2 cm • Borders- • Diaphragmasellae (dural fold) • Lateral sinuses • Sphenoid sinuses • Contiguous to vascular and neurologic structures • Cavernous sinuses • Cranial nerves • Optic chiasm • Hypothalamic neural cells synthesize specific releasing and inhibiting hormones • Secreted directly into the portal vessels of the pituitary stalk • Blood supply derived from the superior and inferior hypophyseal arteries
Anatomy of Chiasm • Relatively radiosensitive in comparison with other CNS tissue. • Located on avg 1 cm above the pituitary, anterior to the infundibulum. • Avg measurements are 8 mm A-P by 4 mm C-C by 13 mm laterally. • Roughly 2 million nerve fibers pass through this volume. • The optic nerves elevate at a 45° angle relative to the orbital roof, and the chiasm maintains this orientation. • Location is variable, differing by up to a centimeter in the AP direction (pre-fixed, normal, and post-fixed).
FIGURE 33.1. Posterolateral view of the pituitary gland. P, posterior; r, right. 1, Pituitary gland; 2, sphenoid sinus; 3, diaphragm sellae; 4, optic chiasm; 5, chiasmatic cistern; 6, anterior cerebral artery; 7, hypothalamus; 8, third ventricle; 9, dorsum sellae; 10, posterior clinoid; 11, pituitary stalk; 12, sella turcica; 13, cavernous sinus; 14, internal carotid artery; 15, right optic nerve; 16, mamillary body.
Pituitary Gland – “MASTER” Gland Plays a critical role in the regulation of most other endocrine glands in conjunction with the hypothalamus. Secretion is regulated by stimulatory hypothalamic releasing factors or inhibitory factor (dopamine inhibits prolactin release)
Function • Anterior Lobe: • FSH • LH • ACTH • TSH • Prolactin • GH • Posterior Lobe: • ADH • Oxytocin
Pituitary Adenomas • Constitute 10–15% of all CNS tumors • 20-25% of pituitary glands at autopsy have adenomas • Etiology is unknown • Secretory - 70%, Non-secretory – 30% • Patients with Secretory adenomas most frequently present with endocrinopathies; the goal of therapy is normalizing the endocrinopathy and eliminating further lesion growth. • M.C - Prolactinomas (50%), 2ndGH secretory, then ACTHsecretory tumors.
Pituitary Adenoma • Microadenomas < 10 mm – may cause focal bulging • Macroadenomas > 10 mm – problems due to mass effect.
Clinical Presentation • M.C. are endocrine abnormalities – hyper-/hypo secretion of ant. pituitary hormones • Headaches • Vision changes – bitemporal hemianopsia and superior temporal defects
Endocrine-Active Pituitary Adenomas • Prolactin– Amenorrhea, Galactorrhea, Impotence • Growth hormone– Gigantism and acromegaly • Corticotropin – Cushing’s disease, Nelson’s syndrome post adrenalectomy • TSH - Hyperthyroidism
Prolactinoma Most common functional pituitary tumors accounting for ~30-50% of all adenomas. Prolactin secretion is extremely efficient; a microscopic adenoma can produce enough prolactin to produce symptoms. Prolactin production Proportional to tumor size Convenient method for monitoring recurrence Inhibited by dopamine (interrupted by head injury or drugs -psychotropics, may be associated with estrogen therapy) can also result in hyperprolactinemia. Symptoms of hyperprolactinemia Amenorrhea–25 % of 2°amenorrhea Galactorrhea Loss of libido Infertility
Prolactinoma • Essential to rule out secondary causes!! • Drugs which decrease dopamine stores • Phenothiazines • Amitriptyline • Metoclopramide • Factors inhibiting dopamine outflow • Estrogen • Pregnancy • Exogenous sources • Hypothyroidism • If prolactin level > 200, almost always a prolactinoma (even in a nursing mom) • GnRH release is decreased in direct response to elevated prolactin, leading to decreased production of LH and FSH
Prolactinoma - Treatment • Medical • Cabergoline – dopamine receptor agonist • Bromocriptine - dopamine agonist • Safe in pregnancy • Will restore menses • Decreases both prolactin and tumor size (80%) • Surgical • Transsphenoidal surgery • Radiotherapy
Somatotroph Adenomas 2nd M.C pituitary adenoma 20 production of somatomedins (ILGF-1, somatomedin C) and GH result in end-organ effects. Gigantism- Prior to bone maturity. Generalized increase in body size, long limbs and hypogonadism Hypersecretion of GH -> hepatic secretion of insulin-like growth factors Acromegaly- After bony maturity. Enlargement of the head, hands, feet, jaw, tongue and soft tissues resulting in characteristic features. Excess GH -> HTN, Diabetes and accelerated atherosclerotic cardiovascular disease.
Acromegalics suffer end-organ effects from hypertension & abnormal glucose metabolism
Somatotroph Adenomas • Diagnosis • Screen: • Check for high IGF-I levels (>3 U/ml) • Remember, levels very high during puberty • Confirm: • 100gm glucose load • Positive: GH levels do not increase to <5ng/ml • Treatment • Surgical • Radiation • Bromocriptine - temporizing measure • May decrease GH by 50% • Octreotide • For suboptimal response to other treatment
Cushing’s disease • Proximal muscle wasting & weakness • Osteoporosis • Glucose intolerance • HTN, hypokalemia • Thromboembolism • Depression, Psyc • Infection • Glaucoma • Centripetal obesity • Moon face; buffalo hump • Skin atrophy • Easily bruised • Striae • Cutaneous fungal infections • Hyperpigmentation • Oligo or amenorrhea • Hirsutism and Virilization with adrenal tumors
Lactotroph adenoma of the Pituitary can develop during pregnancy.
Posterior Pituitary Syndromes Consists of the supra-optic and para-ventricular nuclei (Hypothalamus) Inappropriate oxytocin production has not been associated with any clinical abnormalities ADH- control of water conservation by the kidney. ADH deficiency (diabetes insipidis) excessive urination due to the inability to resorb water -> polydipsia and hypernatermia. Syndrome of inappropriate ADH secretion (SIADH) Resorption of excessive amounts of water resulting in hyponatremia ->seizures, cerebral edema, coma and death. Most frequent cause - secretion by malignant neoplasms (a paraneoplastic syndrome) Most often associated with SCLC, non-malignant lung processes & head injuries
Non-functioning Adenomas • 25-30 % of pit. adenomas do not have classical hyper-secretorysyndr • May grow to a large size before they are detected • Present due to mass effect • Visual deficits • HA • Hormone deficiency- Gonadotropin Deficiency-Loss of libido, Infertility, Loss of secondary sex characteristics
ACTH Deficiency • Results in hypocortisolism – Malaise, Anorexia, Weight loss, GI disturbances, Hyponatremia, Unable to tan or maintain a tan • No features of mineralocorticoid deficiency (Aldosterone secretion unaffected) TSH Deficiency • Hypothyroidism & Atrophic thyroid gland Prolactin Deficiency • Inability to lactate postpartum • Often 1st manifestation of Sheehan syndrome Growth Hormone Deficiency • Adults-Often asymptomatic, may complain of fatigue, decreased exercise tolerance, abdominal obesity, loss of muscle mass • Children- GH Deficiency, Constitutional growth delay
Hypopituitarism Caused by disorders that result in decreased section of pituitary hormones due to disorders of the pituitary itself or the hypothalamus. The pituitary is robust and ~75% of the parenchyma must be destroyed before symptoms occur. Causes: Tumors and mass lesions Pituitary surgery and/or radiation Rathke cleft cyst Pituitary apoplexy – acute hemorrhage Ischemic necrosis associated with precipitous hemorrhagic events, DIC, sickle cell anemia, trauma, increased ICP. Empty sella syndrome – anything that results destruction of part or the entire gland 1. Primary: due to a defect in the diaphragma sellae or increased ICP allowing the encroachment of arachnoid and CSF into the sella and compressing the gland. 2. Secondary: due to intervention for a pituitary process usually adenoma which results in the destruction/removal of the pituitary. May be secondary to hypothalamic failure.
Multiple Endocrine Neoplasia (Autosomal Dominant) • MEN Type 1 / Werner’s Syndrome MEN-1 gene locus on chr 11 4 P’s: • Parathyroid Adenoma • Pancreatic Islet cell Adenoma • Pituitary Adenoma • Peptic Ulcer’s (Gastrinoma- Zollinger-Ellison Syn) • MEN Type 2A / Sipple’s Syndrome • Medullary Thyroid Cancer (MTC) – RET proto-oncogene • Pheochromoctyoma • Parathyroid hyperplasia – Primary Hyperparathyroidism ...3 X more common than MEN 2B
MEN 2B or 3 • MTC – more aggressive than MEN2A • Distant mets reported as early as 1st year of life • Pheochromocytoma • NO hyperparathyroidism • Characteristic Phenotype • Marfanoid habitus (no ectopia lentis or aortic abnormalities) • Mucosal neuromas – Puffy lips and bumpy tongue • Hyperflexible joints • Ganglioneuromas • Often located in intestines/colon –> severe constipation and megacolon
Evaluation of Pituitary Adenomas • MRI, Skeletal survey • Cranial Nr Exam, Visual field assessment • Biopsy may be needed for non-secretory tumors to diff it from others on the list • Endocrine evaluation • Special stimulation and suppression tests • Hormone levels
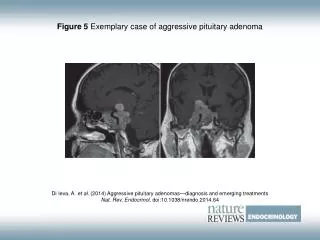
Post-contrast coronal T1 Wtd MRI Post-contrast sagittal T1 Wtd MRI A homogeneously enhancing tumor is seen within the sella (yellow arrows) with suprasellar extension (red arrows) producing optic chiasm compression.
CRANIOPHARYNGIOMA 6.2. Post-contrast sagittal T1 Wtd MRI • Common suprasellar tumor in a child • Tumors can be cystic/solid • A large cystic suprasellar tumor (yellow arrow) with a rim of peripheral enhancement (red arrow). • Common calcified tumor, calcification within the tumor can be seen as high as 90%
General Management • Multidisciplinary approach – Surgeon, Radiation-Oncologist, Endocrinologist. • Goals: • Define tumor extent • Evaluate hormone activity • Remove tumor mass • Control hypersecretion • Correct endocrine deficiencies • Observation: Some series <5% progression • Microadenomas: Transsphenoidal surgery or RT • Macoradenomas: Initial surgery with post-op RT • Medical Management : Bromocriptine, Somatostatin
Microsurgery • Was the gold standard for treatment of sellar lesions. • Advantages: Pathological confirmation, immediate decompression of the optic apparatus, and rapid reduction of hormone over-secretion. • Initial approach is trans-labial or trans-nasal • Trans-sphenoidal resection is currently the most widely used approach. • Trans-cranial approach remains a viable alternative for sellar lesions with extensive supra- or para-sellar extension. • Overall, microsurgery alone provides long-term tumor control rates of only 50 to 80%.
Transcranial Approach • Requires craniotomy and retraction of the frontal lobes of the brain. • Sub-optimal exposure of inferior and posterior aspects of tumor. • Difficult to distinguish normal gland from tumor from distal perspective. • Forces surgeon to operate between CN I or over orbit risking injury to vision or sense of smell. • Used for large invasive tumors or tumors with significant suprasellar extension. • Often used as a combined second stage approach following a transsphenoidal resection.
Microscopic Transseptal-transsphenoidal vs. Endoscopic Transnasal-Transsphenoidal Pituitary Adenoma Resection
Fully Endoscopic Transnasal-Transsphenoidal Pituitary Adenoma Resection (New Gold Std) • A safer operation: • Improved visualization of surrounding optic bulbs, brainstem, and carotid prominences. • Improved ability to differentiate tumor from normal pituitary tissue. • Completely transnasal approach avoids the risk of naso-oral fistulae, and lip numbness seen with the transseptal approach. • A more complete operation: Improved visualization sellar and parasellar tumor extension, results in more complete resections and thus a lower recurrence rate. • Minimally invasive approach allows for a more rapid recovery with less post-operative discomfort: Most patients discharged within 48 hours.
Univ of Toronto, Neurosurgery, 2008 • Remission results: for pts with functioning adenomas - 71% for GH secreting, 81% for ACTH-secreting, and 88% for Prl-secreting adenomas. • This compares with similar results reported
Radiation Therapy • Treatment of pituitary adenomas with radiation dates back to the early 1900s • From the late 1950s to the 1980s, pituitary adenomas were treated with proton and heavy-ion radiosurgery at several laboratory-based treatment centers abroad and in the United States at Harvard Cyclotron Laboratory and Lawrence Berkeley Laboratory • Gramegna A. Un cas d’acromegalie traité par la radiotherapie, Rev Neurol 1909;17:15 • Proton-Beam Therapy in Acromegaly, Kjellberg et al, NEJM, 1968 • - Reported their early experience in 22 pts with acromegaly
RT after Surgery ? • RT can be administered postoperatively as adjuvanttherapy to inhibit recurrent growth or laterwhen biochemical levels, clinical symptoms or neuro-imaging findings indicate a recurrence. • May also be used post-operatively to treat known residual tumor following incomplete or sub-total resection (STR). • The presence of residual tumor is not uncommon in cases of adenomas with either a supra-sellar component or cavernous sinus involvement • Incidence of recurrence has also been shown to correlate with dural invasion by a pituitary adenoma
SRS vs FxRT, Which is better? • Histo-pathological evaluation of pituitary adenoma specimens following either radiosurgery or fractionated radiation therapy is consistent with the notion of a more potent radiobiological effect of radiosurgery. • Radiosurgery also appears to lead to faster normalization of hormone levels than fractionated radiotherapy, further supporting the notion of greater radiobiological potency • When the adenoma is too large (~>3.5cm) to administer an effective dose in a single session without undue risk of complications, fractionated radiotherapy may be more appropriate. • If the tumor is very close (<3 mm) to the optic apparatus, it may be impossible to achieve an acceptably sharp falloff gradient using radiosurgery despite the aid of shielding.
The long-term efficacy of conservative surgery and radiotherapy • Retrospective study of 411 patients treated with EBRT for pituitary adenomas • Goal was to assess both long-term efficacy and toxicity of conservative surgery and RT • 252 of 411 pts with non-functioning pituitary adenomas • 131 of 411 pts had functional adenomas (62 acromegaly, 60 prolactinomas, 7 Cushing’s, 1 TSH, 1 Gn secreting) • 338 had surgical intervention; 11-complete resection • 187 transfrontal approach, 24 trans-sphenoidal approach, 35 had no surgery • Median f/u of 10.5 yrs Royal Marsden - M. Brada et al, Clinical Endocrinology (1993) 38, 571-578