Download

1 / 40
430 likes | 890 Views
Pituitary Disorders. Jo Choudhry, M.D. PGY-1. The Pituitary Gland. Located at the base of the skull Anterior and Posterior lobes Portal connection from the hypothalamus. Growth hormone (GH) Gondadotrophs (LH/FSH) TSH Prolactin Corticotropin (ACTH). Oxytocin Vasopressin.

E N D
Pituitary Disorders Jo Choudhry, M.D. PGY-1
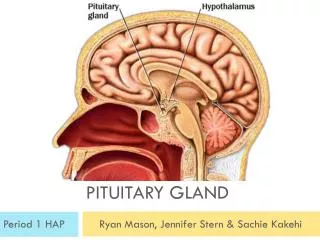
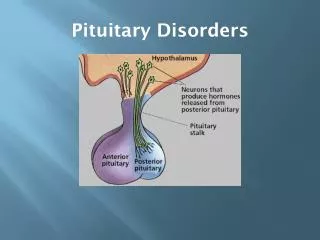
The Pituitary Gland • Located at the base of the skull • Anterior and Posterior lobes • Portal connection from the hypothalamus
Growth hormone (GH) Gondadotrophs (LH/FSH) TSH Prolactin Corticotropin (ACTH) Oxytocin Vasopressin Anterior Lobe Posterior Lobe
Normal Changes in Pregnancy • Anterior lobe size doubles-triples due to lactotrophs. • Placental estrogens stimulate lactotroph proliferation • Decreased response to GnRH, dec. LH/FSH • Decrease pituitary GH, inc. placental GH • Increase CRH (prob. Placental origin) during 2 & 3 trimesters • 2-4 X increase in ACTH, despite inc. in bound and free cortisol.
Hyperprolactinemia • Causes: • 1. disruption of dopamine (tumor, trauma, infiltrative lesions) • 2. hypothyroid (increases TRH) • 3. estrogen increase (pregnancy) • 4. chest wall burns – nueronal effect like suckling • 5. chronic renal failure, returns to nml after transplant • 6. drugs (verapamil, H2 blockers, estrogens, opiates, dopamine receptor antagonists, reserpine, a-methyldopa)
Prolactinomas • Most common functional pituitary tumor • 10% are lactotroph and somatotroph such as GH producing • Presents with amenorrhea and infertility • Prolactinomas lose TRH response • Microadenomas <10mm on MRI • Macroadenomas >10mm
Treat only if symptomatic (HA, vision changes) Dopamine agonist (Bromocriptine) 1.25mg qhs 1 wk, then BID If intolerant with nausea, may give vaginally Not recommended for breastfeeding Transspenoidal surgery if unsuccessful Treatment Pregnancy Not Desired
Risks of surgery: *4.6% post-op neurologic complication: infarction/hemorrhage *2-10.5% Diabetes Insipidous *8.8% fluid and electrolyte *2% Cerebrospinal fluid rhinorrhea *2% Meningitis *3.2% cranial nerve 3,4,or 6 palsies
Treatment Pregnancy Desired • If macro, shrink size b/f preg with bromocriptine (36% will develop neurologic symptoms) • If causing major visual defect and unresponsive, consider transspenoidal surgery b/f preg. • Bromocriptine until preg occurs, then stop.
During Pregnancy • Visual field check q2-3 mos. and MRI prn • If neurologic symptoms occur during preg, usually about 14wga, restart treatment. • Class B • If severe and unresponsive: • 2nd trimester: consider surgery • PTL risk • 3rd trimester: wait until PP
Acromegaly • 98% GH pituitary adenoma • 1/3 of all functional pituitary adenomas • Stimulates growth of skin, connective tissue, cartilage, bone, and viscera • Nitrogen retention, insulin antagonism, and lipogenesis
Arthropathy Neuropathy Cardiomyopathy Respiratory obstruction Diabetes Mellitus Hypertension: exaterbates cardiomyopathy NOT Reversible increased risk of tumors: leiomyomata colon polyps Risks of Long Term Excess GH Reduced overall survival by an average of 10 years
Diagnosis • Somatomedian-C levels and IGF-1 levels • If pregnant: special assay to distinguish placental GH • 70% pitutary GH responds to TRH, placental variant does not.
Treatment • Goal: lower the serum insulin-like growth factor to normal for age/gender • Surgically accessible micro- or Macroadenomas: • Transspenoidal surgery • 2nd Line therapy: Somatostatin analogs or Dopamine agonists • 3rd Line therapy: Somatostatin receptor antagonist • Last resort: Radiation
Pregnancy and Acromegaly • D/C tx with confirmation • GH Maternal to Fetal transfer negligible, except for glu intolerance. • If severe neurologic sympts, try Bromocriptine • May not dec. GH, shrink lactotrophs • Somatostatin analogs have been used in 3 pts with no ill effects to fetus, despite transplacental passage.
Cushing’s Disease • High ACTH leads to excess glucocorticoid • Incidence may be 5-25 per million • Women are 3-8X more likely than men
Cushing’s disease • Centripetal obesity • Moon face; buffalo hump • Skin atrophy • Easily bruised • Striae • Cutaneous fungal infections • Hyperpigmentation • Oligo or amenorrhea • Hirsutism and Virilization with adrenal tumors
Cushing’s Disease • Proximal muscle wasting & weakness • Osteoporosis • Glucose intolerance • HTN, hypokalemia • Thromboembolism • Depression, Psyc • Infection • Glaucoma
Complications if Pregnant Rare due to decreased fertility • Premature birth • SAB, Stillbirths • IUGR • Neonatal adrenal insufficiency • Maternal: HTN, DM, CHF, Death
Diagnosis Cushing’s Syndrome: • 24 hr urine cortisol excretion • If not 3x nml, measure pm salivary cortisol Cushing’s Disease vs. Syndrome: • HIGH dose Dexamethasone suppression test (8mg overnight) • Successful if Pituitary origin
Treatment • Transsphenoidal surgery • Pituitary irradiation • Adrenalectomy (Surgical, Mitotane) • Nelson’s Syndrome: expanding intrasellar tumor and hyperpigmentation • Pregnancy: • 1st Trimester: Surgery • 2nd Trimester: Adrenal Enzyme Inhibitors vs. surgery • 3rd Trimester: Early delivery, enzyme inhibitors until lung maturity
Thyrotropin-secreting Adenoma • <1% of all hyperthyroidism cases • 25% of adenomas secrete other hormones • Goiter, visual defects, menstral irreg, galatorrhea Lab: Normal or High TSH High total and free T4 and High T3 MRI
Treatment • Transsphenoidal surgery • 1/3 Cure • 1/3 improvement • 1/3 no change • Dopamine Agonist • Somatostatin Analogue (Octreotide) • Works so well, may give before surgery • Nausea, diarrhea, bloating, glu intolerance, cholelithiasis • Do NOT use antithyroid therapy
Gonadotroph adenoma • Usually considered non-functioning • Secrete inefficiently, variably • Presents with nuerologic symptoms • Difficult to Diagnose • Rule out other adenomas • Prepubertal girls= breast devel, vag. Bleeding • Premenopausal= amenorrhea, oligo
Gonadotroph adenoma vs. menopause and ovarian failure • High FSH with low LH • High serum free alpha subunit • High estridiol, FSH, thickened endometrium and polycystic ovaries
Treatment of non-functioning and gonadotrophin macroadenomas • Transsphenoidal surgery • +/- Radiation
Hypopituitarism • 76% tumor or treatment of tumor • Mass effect of adenoma on other hormones • Surgical resection of non-adenomatous tissue • Radiation of pituitary • Check hormones 6 mos after and then yearly • 13% extrapituitary tumor • Craniopharyngioma • 8% unknown • 1% sarcoidosis • 0.5% Sheehan’s syndrome
Infiltrative Lesions • Hereditary Hemochromatosis • Fe deposition in pituitary • Gonadotropin deficiency most common • Tx repeat phlebotomy • Pituitary Apoplexy • Sudden hemorrhage into pituitary • Severe, sudden HA; diplopia; hypopituitarism • Sudden ACTH def. is life-threatening hypotension • Tx: surgical decompression
Sheehan Syndrome • Infarction of Pituitary after substantial blood loss during childbirth • Incidence: 3.6% • No correlation between severity of hemorrage and symptoms • Severe: recognized days to weeks PP • Lethargy, anorexia, weight loss, unable to BF
Sheehan’s Syndrome • Typically long interval between obstetric event and diagnosis • Of 25 cases studied: • 50% permanent amenorrhea • The rest had scanty-rare menses • Most lactation was poor to absent • Dx: MRI empty sella turcica
TX with hormones 87% live births 13% SAB 0 Stillbirths 0 Maternal deaths Don’t TX 58% live births 42% SAB 1 Stillbirth 3 Maternal deaths Sheehan’s and Pregnancy Labor: HYDRATION!! IV Cortisol: adjusted for pt’s state 25-75mg q6 hr
Lymphocytic Hypophysitis • 22 y/o female died of circulatory collapse 8 hours after appy. She was 14 mos. PP and had developed 2nd amenorrhea. Autopsy: lymphocytic infiltration of pituitary and thyroid Symptoms: HA, lethargy, weight loss, hyperprolactinemia
Lymphocytic Hypophysis • Scheithauer et al, ’90 • 69 women that died during preg or PP • 5 had the disease, 4/5 died at 38-41 wga • Consider especially if no hemorrhage • TX: HRT (thyroid, cortisol)
Pituitary Necrosis • Pregnant Diabetic Patients • Due to vascular changes • DX: severe, midline HA and vomitting in 3rd trimester followed by decrease of insulin requirements • 3/8 cases reported: assoc. with fetal and then maternal death
Polydipsia and Polyuria (2-15 Liters/day) Abrupt onset 30-50% are idiopathic Dec. production by hypothalamus Surgery or Trauma Rare with Sheehan’s Mild, undetectable degree Central Diabetes Insipidus
Dx of Central DI • Water Deprivation test: • Restrict p.o. fluids or administer hypertonic saline to increase serum osmolality to 295-300 mosmol/kg (nml: 275-290) • Central DI: urine osmolality still low and returns to normal after administer vasopressin • Nephrogenic DI: exogenous vasopressin does not alter urine osmolality much
Pregnancy and Central D.I. • Transient D.I. during pregnancy due to acquired or hereditary D.I. • Latent: Unable to sustain during pregnancy • Transient Arginine Vasopressin resistant, but L-Deamino, 8-D-arginine vasopressin (DDAVP=Desmopressin) responsive • High amounts of placental vasopressinase • D.I. antedates pregnancy. Most deteriorate due to vasopressinase
Treatment of Central D.I. • DDAVP (Desmopressin Acetate) • Synthetic analog • Not catabolized by vasopressinase • No vasopressor action • Administered intranasally (rec.) or p.o. • Titrate 10-20ug qd or bid • Safe in pregnancy and breastfeeding
References • Saunders; Maternal-Fetal Medicine 5th Edition; Chapter 51 ppg. 1083-1094. • Weiss, R; Refetoff, S; Thyrotropin Secreting Pituitary Adenomas; Up To Date online Jan. 2005; www.uptodate.com • Synder,P.; Clinical Manifestations and diagnosis of gonadotroph and other clinically nonfunctioning adenomas; Up To Date online; Jan. 2005; www.uptodate.com • Barker,F; Klibanski,A; Swearingin,B; Transsphenoidal Surgery for Pituitary Tumors in the United States, 1996-2000: Mortality, Morbidity, and the Effects of Hospital and Surgeon Volume; Journal of Clinical Endocrinology and Metabolism Vol. 88, No. 10, ppg. 4709-4719. • Nieman, L; Orth, D; Clinical manifestations of Cushing’s Syndrome; Up To Date online; Jan. 2005; www.uptodate.com • Nieman, L; Orth, D; Treatment of Cushing’s Syndrome: Diminishing adrenal cortisol synthesis. Up To Date online; Jan. 2005; www.uptodate.com • Synder, P; Abrahamson, M; Management of lactotroph adenoma (prolactinoma) during pregnancy; Up To Date online; Jan. 2005; www.uptodate.com • Melmed, S; Treatment of Acromegaly; Up To Date online; Jan. 2005; www.uptodate.com • Melmed, S; Clinical manifestations of acromegaly; Up To Date online; Jan. 2005; www.uptodate.com • Synder, P; Treatment of Hypopituitarism; Up To Date online; Jan. 2005; www.uptodate.com • Abrahamson, M; Synder, P; Causes of hypopituitarism; Up To Date online; Jan. 2005; www.uptodate.com • Garner, P. Pituitary Disorders of Pregnancy; Endotext.com; Chapter 2A; March 2002. • Rose, B.; Causes of Central Diabetes Insipidous; Up To Date online; Jan. 2005; www.uptodate.com • Rose, B.; Treatment of Central Diabetes Insipidous; Up To Date online; Jan. 2005; www.uptodate.com • Rose, B; Diagnosis of polyuria and Diabetes insipidus; Up To Date online; Jan. 2005; www.uptodate.com