Download
1 / 16
160 likes | 258 Views
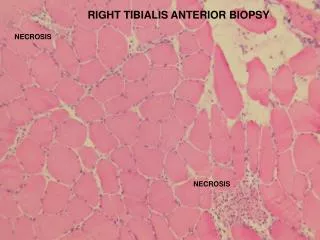
Anesthesia for a Muscle Biopsy. Alyssa Brzenski. Case .

E N D
Anesthesia for a Muscle Biopsy Alyssa Brzenski
Case You are assigned to do an anesthetic for a muscle biopsy. The patient is a 13 month old male toddler with delayed motor milestones. He can not sit unsupported, roll over, cruise or walk yet. He was delivered at 35 weeks PCA and spent 1 week in the NICU for feeding difficulties. There were never any respiratory difficulties. Per the parents the toddler has not had any prior anesthetics. There is no family history of muscular weakness or any problems with anesthesia although mom tells you that she was adopted and knows nothing about her biological family.
What are you going to do? • Are there any questions you would like to ask? • What are your concerns? • What is your anesthetic plan?
MH Susceptible Diseases King Denborough Syndrome with and without mutations. Neuromuscular Disorders. Vol 21, Iss 6, June 2011 420-7.
TIVA for muscle biopsy • What are baseline goals for all patients with mitochondrial myopathies? • Should a TIVA be used then? • How would a propofol based TIVA affect the child with mitochondrial myopathies?
Types of Mitochondrial Myopathies • Types of Mitochondrial Myopathies • Respiratory chain deficiencies • Mitochondrial DNA mutations • Mitochondrial deletions
Anesthetic Goals of Mitochondrial Myopathies • Understand the disorder • Reduced fast • IV fluids with glucose and avoids lactate • Avoid stress that can aggravate energy production • Monitor acid-base status • Maintain temperature • Maximize pain relief
Why avoid Propofol? • All anesthetics depress mitochondrial function • Propofolinhibits mitochondrial function at complex I, uncouple oxidative phosphorylation and is associated with propofol infusion syndrome • Patients with mitochondrial disease are at increased risk for toxic effect, namely cardiac depression and respiratory failure (during surgery and later).
Sources 1. Allison KR: Muscular dystrophy versus mitochondrial myopathy: the dilemma of the undiagnosed hypotonic child. PaediatrAnaesth 2007; 17: 1-6 2. Benca J, Hogan K: Malignant hyperthermia, coexisting disorders, and enzymopathies: risks and management options. AnesthAnalg 2009; 109: 1049-53 3. Davis PJ, Brandom BW: The association of malignant hyperthermia and unusual disease: when you're hot you're hot or maybe not. AnesthAnalg 2009; 109: 1001-3 4. Driessen J, Willems S, Dercksen S, Giele J, van der Staak F, Smeitink J: Anesthesia-related morbidity and mortality after surgery for muscle biopsy in children with mitochondrial defects. PaediatrAnaesth 2007; 17: 16-21 5. Driessen JJ: Neuromuscular and mitochondrial disorders: what is relevant to the anaesthesiologist? CurrOpinAnaesthesiol 2008; 21: 350-5 6. Footitt EJ, Sinha MD, Raiman JA, Dhawan A, Moganasundram S, Champion MP: Mitochondrial disorders and general anaesthesia: a case series and review. Br J Anaesth 2008; 100: 436-41 7. Gurnaney H, Brown A, Litman RS: Malignant hyperthermia and muscular dystrophies. AnesthAnalg 2009; 109: 1043-8 8. Klingler W, Rueffert H, Lehmann-Horn F, Girard T, Hopkins PM: Core myopathies and risk of malignant hyperthermia. AnesthAnalg 2009; 109: 1167-73