Download
1 / 37
400 likes | 854 Views
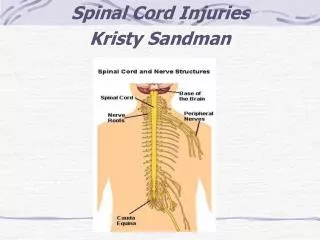
Spine and spinal cord injuries. Spine and spinal cord injuries mechanisms of spine injuries. flexion injury extension injury axial loading rotation injury. Spine and spinal cord injuries mechanism. flexion injury Cervical and thoracic spine thoracolumbar junction

E N D
Spine and spinal cord injuriesmechanisms of spine injuries • flexion injury • extension injury • axial loading • rotation injury
Spine and spinal cord injuriesmechanism • flexion injury • Cervical and thoracic spine thoracolumbar junction • Vertebral body fracture with anterior wedging • extension injury • Cervical spine ! • Fractures of posterior elements (posterior column), with ligaments disruption subluxations and spodylolisthesis • NOTE! In this mechanism the spinal cord injury and root compression may occur without evident osseous changes visible on plain films
Spine and spinal cord injuriesmechanism • axial loading • C spine – diving L-S spine – jumping • compression („burst”) fractures of vertebral bodies lateral element (processes fractures) and articular pillar fractures • rotation injury • Usually in combination with flexion-extension injury • Lateral mass fractures, luxations, uncovertebral dislocations
Spine and spinal cord injurieseffects • oseous changes, fractures • posttraumatic instabilities and spondylolistheses • posttraumatic disc herniations • spinal cord contusion • spinal cord compression • vascular spinal cord injury
Spine and spinal cord injuries • Osseous changes – most important sings • atlantooccipital dislocation • common, but not always fatal • on lateral plain film: dens – basion distance > 12,5 mm • most common to C1 is a bilateral vertical fracture through the neural arch = aJefferson fracture = a burst fracture that involves both anterior and posterior arches
Jefferson fracture – of C1 anterior and posterior arches : The burst mechamism causes the lateral displacement of the lateral parts of C1 Posterior arch C1 fracture
Odontoid – dense fracture C2 fracture, is often combined with luxation of C1 – may efect with spinal cord compression; CT with MPR and 3D reconstructions is advisable
Flexion-extension mechanism: avulsion fracture C5 spinous process fracture C7 C 2 on CT C 5 C 7
rotation mechanism: C1- posterior arch, body of C2 and odontoid fractures - luxation
Spine and spinal cord injuries • Osseous changes – most important sings • Odontoid (dens) fractures • Usually at the base of dens – poorly visible on axial CT – MPRs and 3Ds necessary! • Hangman’s fracture bilateral transpedicle with the separation of neural arch from the vertebral body and spondylolisthesis, dens and ligaments are usually intact
Transverse C2 body fracture – Hangman’s fracture - with bilateral arch-body separation – the result is instability
C2 dens apex fracture visible on 3D SSD! Spinal canal stenosis can be evaluated
Spine and spinal cord injuries • Osseous changes – most important sings • C1-C2 luxations • in all methods:plain films,CTand MR: • normal distance between anterior arch of C1 and dens of C2 is 1 to 3 mm • distances between dens and lateral masses of C1 should be • equal • luxation – spondylolisthesis is important when larger than • 3-4 mm • NOTE ! Arches and processes fractures are common at C6, i C7 and in L-S spine
C1-C2 luxation plain film(Rheumatoid arthritis) malum suboccipitale > 3 mm
C1-C2 luxation MR T1w(Rheumatoid arthritis) malum suboccipitale
C1-C2 luxation MR T2w(Rheumatoid arthritis) malum suboccipitale
Body and arches of C2 + arches of C3, luxation (CT MPR and 3D SSD)
Spine and spinal cord injuries • Osseous changes – most important sings • Compression („burst”) and multifragment fractures of vertebral bodies may cause free osseuos fragments protrusion to the spinal canal, resulting with spinal cord damage or/and compression • free or protruding osseous fragments are well seen on CT especially with MPRs and 3D SSD reconstructions • Spiral or multislice CT can be used to evaluate the spinal canal stenosis caused by fractures or spondylolistheses and precisely define the location of the most threatening fragments
Spine and spinal cord injuries Posttraumatic spinal cord compression is caused by: · haematoma - epidural - or inside the cord · disc herniation · spondylolisthesis or luxation · osseous fragments
Spine and spinal cord injuries ·CT visualize - osseous changes - spinal canal stenosis - disc herniation - rarely haematoma
Spine and spinal cord injuries • · MR visualize • - cord oedema • haematoma, contusion, vascular injury • - disc damage and herniation • - osseous changes are poorly visualized on MR - use CT! • - Instead MR perfectly visualizes spinal cord displacement, compression and focal lesions !
Spine and spinal cord injuries Spinal cord contusion · bleeding foci within the cord grey matter - best visible on MR - on CT visible while massive - on CT hyperdense foci inside the cord (60 – 70 HU) - on MR image is phase dependent
Spine and spinal cord injuries Spinal cord contusion MR # acute phase 1- 4 days – slightly hyperintense on T2w, hypointense w T1w # subacute phase 2-4 days up to 3 weeks – slightly hyperintense on T2w, hyperintense on T1w # chronic phase more than 3 weeks – strongly hyperintense on T1 & T2w, accompanied by: - oedema – high signal on T2w - malacia – inhomogenous, high signal on T2w # residual – glial scar and myelomalacia
Spine and spinal cord injuries vascular spinal cord injury - caused by compression, vasospasm or damage of the spinal vessels - resulting ischaemia leeds to necrosis and myelomalacia - Well seen onMR: hypointense on T1w and hyperintense on T2w