Download

1 / 10
130 likes | 503 Views
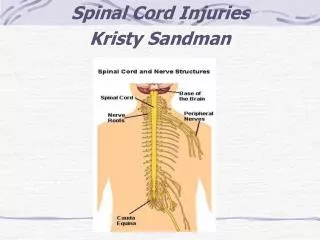
Spinal Cord Injuries. Spinal Cord. SC extends from the foramen magnum to the lower border of the first lumbar vertebra, where it reaches a conical termination, the conus medullaris Vertebra - 7 Cervical vertebra, 12 Thoracic vertebra, 5 Lumbar vertebra, 5 Sacral vertebra, Coccyx

E N D
Spinal Cord • SC extends from the foramen magnum to the lower border of the first lumbar vertebra, where it reaches a conical termination, the conusmedullaris • Vertebra • - 7 Cervical vertebra, 12 Thoracic vertebra, 5 Lumbar vertebra, 5 Sacral vertebra, Coccyx • Spinal nerves • - 8 Cervical nerves, 12 Thoracic nerves, 5 Lumbar nerves, 5 Sacral nerves, 1 Coccygealnerve • Landmarks • - Inferior angle of the scapula: T7, Iliac crest: L4, Vertebra prominens: C7
Spinal Cord Injuries • Mechanism of Injury • - any force that causes movement beyond the physiologic limits • Less common in children than in adults • Causes of Traumatic Spinal Cord Injury • Road traffic accidents • - Domestic & industrial accidents • - Sports injuries • - Self-harm & assault
Spinal Cord Injuries Complete lesion Absence of sensory/ motor function in the lowest sacral segments Incomplete lesion Either sensory/ motor function is preserved (Sacral sparing)
Signs and Symptoms • Cardiovascular – arrhythmia, bradycardia • Orthostatic hypotension - lightheadedness, dizziness, syncope • Deep venous thrombosis/ Pulmonary embolism • Autonomic dysreflexia • Pulmonary – decreased forceful expiration/ cough, pneumonia • Spasticity • Pain • Neurogenicbladder/ bowel
Clinical Syndromes in Spinal Cord Injury • Anterior Cord Syndrome - Affects anterior spinal cord & preserves posterior columns - Variable loss of pinprick & temperature sensation - Spared propioception - Due to trauma to anterior aspect of spinal cord or anterior spinal artery • Central Cord Syndrome - Sustained hyperextension - Occurs in the cervical area - Motor weakness is greater in the upper extremities than in the lower extremities - Varying bowel/ bladder/ sexual dysfunction • Brown-Sequard Syndrome - Hemisection of the spinal cord - Relatively greater ipsilateralpropioceptive & motor loss - Contralateralloss of sensation to pinprick & temperature • Conusmedullaris Lesion - Areflexic bladder/ bowel & flaccid lower extremities paralysis - Spinal cord ends as conusmedullaris at L1 • Cauda equine lesion - Lower motor neuron lesion - Bowel/ bladder/ lower extremities flaccid paralysis
Diagnosis • Physical Examination - Starts from head to toe - Know the dermatomes and mytomes to localize injury without the use of x-ray - Complete neuro exam- motor and sensory deficit - If patient is unconscious, check for withdrawal from pain to localize
Diagnosis • Imaging Procedures - X-rays- AP lateral views (2nd view has to be taken at right angle to the first) - CT scan - MRI
Management • Starts at the scene of injury • Address life-threatening problems first • ABCs of management • Golden period for Tx: 8 hours Increase in tissue epinephrineischemia of SCnerve tissues are edematous, etc irreversible injury - give steroids and SC cooling • Immobilization: cervical collar
Neuro exam- 3 L’s (levelize, lateralize, localize) • Definitive management • Supportive: nasogastric decompression, catheter drainage of bladder, avoidance of postural hypotension • Surgical treatment is required for serious fractures and dislocations, progressive neurological deficits, or wounds. Indicators for urgent surgery are: *neurologic deterioration, ascending paralysis or sensory loss *extremely unstable vertebral injury *spine that cannot be aligned with traction • Preserve remaining functions • Avoid complications of prolonged recumbency i.e. pneumonia, bed sores, UTIs • Maintain physiologic well-being • Rehabilitation initiated at the earliest possible time