Download
1 / 19
190 likes | 330 Views
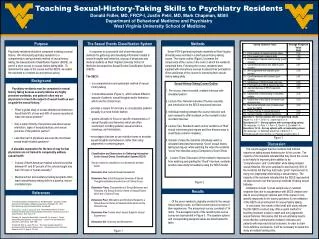
Open Dialogue in Dutch Psychiatry: Will Revolution help or is it just a Fata Morgana?. Goal of the workshop: discuss desirability and possibility of a dialogical approach in the setting of the Outreaching Psychiatric Emergency Service (OPES) in Amsterdam.

E N D
Open Dialogue in Dutch Psychiatry: Will Revolution help or is it just a Fata Morgana? van oenen @ cornelis 2013
Goal of the workshop: discuss desirability and possibility of a dialogical approach in the setting of the Outreaching Psychiatric Emergency Service (OPES) in Amsterdam van oenen @ cornelis 2013
Setting Outreaching Psychiatric Emergency Service (OPES) Amsterdam: • Emergencypsychiatryand (subsequent) brief therapy • Multidisciplinary team • Reasonsforreferral: psychiatric disorders, suicidality, psycho-socialproblems, behavioralproblems, public nuisance • Systemicandpsychiatric approach van oenen @ cornelis 2013
Three different systemic approaches 1) Medical, linear, approach . Therapist asks system for information, diagnoses patient, gives family psycho-education. van oenen @ cornelis 2013
Three different systemic approaches 1) Medical, linear, approach . Therapist asks system for information, diagnoses patient, gives family psycho-education. 2) Consensus oriented Systemic Interviewing and Intervention. Therapist facilitates structure and content of meeting with identified patient and relatives. Part of plan can be psychiatric examination. Result will be discussed. van oenen @ cornelis 2013
Three different systemic approaches 1) Medical, linear, approach . Therapist asks system for information, diagnoses patient, gives family psycho-education. 2) Consensus oriented Systemic Interviewing and Intervention. Therapist facilitates structure and content of meeting with identified patient and relatives. Part of plan can be psychiatric examination. Result will be discussed. 3) Open dialogue approach. Different voices can be heard without psychiatric labelling in open andequalencounter, without preconceivedintentions or stategies. Aim is creating open spacefor new perspectives van oenen @ cornelis 2013
Position of therapist in different approaches van oenen @ cornelis 2013
Position of therapist in different approaches • Medical approach: expert. Directs conversationfrom a controlling position, operates in monologue. van oenen @ cornelis 2013
Position of therapist in different approaches • Medical approach: expert. Directs conversationfrom a controlling position, operates in monologue. • CSII: consultant. Directs andfacilitatesdialogue (‘expert in consultancy’) andparticipatesfrom a ‘semi-equal’ position. van oenen @ cornelis 2013
Position of therapist in different approaches • Medical approach: expert. Directs conversationfrom a controlling position, operates in monologue. • CSII: consultant. Directs andfacilitatesdialogue (‘expert in consultancy’) andparticipatesfrom a ‘semi-equal’ position. • Open dialogue: participant. Facilitatesandparticipates in anequalpostion. Subjectiveexperiencecounts, no framing is offered. van oenen @ cornelis 2013
Historicaldevelopmentsystemicpositions • Starting as an expert in cybernetic, structuralandstrategic school. • Shiftingtowards consultant position in circulair questioningand solution focused school • ‘Ending’ in equal participant in narrativeand open dialogue approach. • (and back…?) van oenen @ cornelis 2013
Thesis 1 • Therapist has to switch betweenpositions, fitting to the client, relativesandspecificsituation van oenen @ cornelis 2013
Thesis 2 • Open dialogue is often not applicable in Outreaching Psychiatric Emergences Service Amsterdam van oenen @ cornelis 2013
Oftennotapplicablebecause: • 1) It does not fit into the Dutch culture of the patient and his relatives: “One is in crisis and wants help from an expert who solves the problem!” • 2) The assurance asks for a psychiatric diagnosis. • 3) Patients are sometimes too ill or too aggressive to have a dialogue. (I.e.: manic patients.) • 4) Feedback (CDOI) worked counterproductive van oenen @ cornelis 2013
Case • Woman, 34 years. • Referral: anxiety, panic, suicidalthoughts. • History: has sufferedfrom severe depession 5 yearsago. • Actualsituation: partner has to move abroadfor job. Client anxiousforreneweddepression. ‘If I get depressedagain, I’drather die’. van oenen @ cornelis 2013
Questions • Whichpositionwouldyou take? • Which goal wouldyoudefineforyourself? • How wouldyouexplainyour approach to the clientandrelatives? van oenen @ cornelis 2013
Case continued • Client: wants to talk about events in the past, stressingneedfor help; concentrationdiminishes, level of anxietyrises. • Partner: asksurgentlyforadvice • No solution comes up. • Whatwouldyou do? van oenen @ cornelis 2013
Question • Whichpositionwouldyou take? • Which goal wouldyoudefineforyourself? • How wouldyouexplainyour approach to the clientandrelatives? van oenen @ cornelis 2013
Thank you… for the attention! van oenen @ cornelis 2013