Download
1 / 28
300 likes | 430 Views
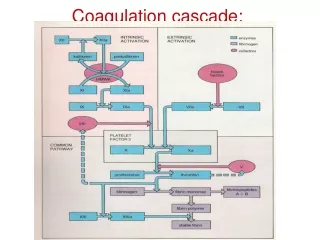
Coagulation. Janet Birchall Consultant Haematologist November 2016. Aim to discuss -. Venous thromboembolism (VTE) DVT, PE - risk of recurrence Happy to discuss other topics – upper limb dvt, cerebral thrombosis, antiphospholipid syndrome

E N D
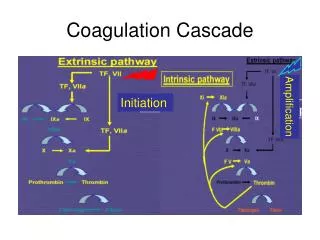
Coagulation Janet Birchall Consultant Haematologist November 2016
Aim to discuss - • Venous thromboembolism (VTE) DVT, PE - risk of recurrence • Happy to discuss other topics – upper limb dvt, cerebral thrombosis, antiphospholipid syndrome • Bleeding problems – which symptoms/signs are significant?
Venous ThromboembolismCASES How would you manage? • 22 yr old male, ilio-femoral DVT • 50 yr old male, posterior tibial vein DVT • 40 yr old male, recurrent proximal DVT • 55 yr old female with antiphospholipid syndrome and unstable INR
Secondary complications of VTE 1. Kahn SR, Ginsberg JS. Arch Intern Med 2004;164:17 -26; 2. McNeil K, Dunning J. Heart 2007;93:1152–8; 3. Pengo V et al. N Engl J Med 2004;350(22):2257–64. • Post-thrombotic syndrome (PTS)1 • Can occur within 1–2 years after DVT in 20% to 50% of all patients • Severe PTS occurs in 25–33% of patients with PTS • Can lead to deep vein insufficiency and leg ulcers • Chronic thromboembolic pulmonary hypertension (CTPH) • Can occur after PE and is associated with significant morbidity and mortality2 • Incidence of CTPH after an acute episode of PE3 • 1.0% at 6 months • 3.1% at 1 year • 3.8% at 2 years
Length of anticoagulation Recurrent Thrombosis Bleeding Decisions made on subjective clinical criteria Risk benefit analysis
Recurrent after cessation anticoagulation at 6 months Idiopathic Non surgical risk factors Surgery last 6 weeks Baglin, Lancet 2003
Relative risk (RR) recurrent VTE
Preceding length of AC & initial presentation on risk of recurrent VTE after stopping treatment • Recurrence and length of AC • if AC stopped < 6/52 compared with > 3/12, HR 1.52 • similar if stopped at 3/12 compared with > 6/12. HR 1.19 • Recurrence position & precipitation Boutitie et al, BMJ, 2011
Initial therapy If isolated calf vein DVT, treatment can be limited to 6 weeks (1A). • Continued anticoagulation • Consider in unprovoked proximal DVT or PE • Cohort risk of recurrence if unprovoked VTE >9%, individual risk heterogeneous. • If stop consider - • D-dimer – lower recurrence if negative compared to those with elevated D-dimer (3.5% vs. 9%) (Verhovsek et al, 2008). • Testing for antiphospholipid antibodies and if positive restarting AC • Risk of recurrence also related to post-thrombotic syndrome (Stain et al, 2005; Rodger et al, 2008) and male sex (Eichinger et al, 2010).
VTE diseases: diagnosis, management CG144. Published June 2012. Updated 2015 Thrombolytic therapy - Iliofemoral DVT Consider if symptoms < 14 days, good functional status, life expectancy of >1 year and low risk of bleeding. - Pulmonary embolism - Consider if haemodynamic instability. Offer VKA if confirmed proximal DVT or PE within 24 hours and continue for 3 months. Investigation for cancer Consider abdomino-pelvic CT scan (and mammogram for women) if > 40 years with 1st unprovoked DVT or PE Continued anticoagulation - Offer VKA > 3/12 if unprovoked PE, taking into account risk of VTE recurrence and risk of bleeding. Discuss with the patient. - Consider VKA > 3/12 if unprovoked proximal DVT if risk of recurrence high and no additional risk of major bleeding. Discuss with the patient.
Bleeding problemsCASES How would you manage? 22 yr old female, spontaneous bruising 40 yr old female, post op bleeding & referred by surgeons 25 yr old female, brushing teeth gum bleeding 55 yr old female with muscle haematoma
bjh guideline The diagnosis and management of von Willebrand disease: a United Kingdom Haemophilia Centre Doctors Organization guideline approved by the British Committee for Standards in Haematology ISTH/SSC bleeding assessment Epistaxis – not signif if < 10 mins duration, < x5/yr, seasonal or assoc with URTI or other identifiable cause. Cutaneous bleeding – Bruising significant if > 5 (>1cm) in exposed areas, petechiae, haematoma without trauma. Minor cutaneous wound – bleeding episode with superficial cut (shaving, knife) or that requires frequent bandage changes. Need to be more than one occasion. Insignificant if <10 mins bleeding duration. Oral cavity – Gum - significant if frankly bloody sputum and lasts > 10mins on > 1 occasion. Tooth eruption or spontaneous loss – medical assistance or bleeds > 10mins. Bites to lips, cheeks, tongue > 10 mins or → swelling . GI bleeding – any unexplained bleeding. Haematuria – macroscopic (ie visible – red/pink) not otherwise explained. Tooth extraction – bleeding after leaves dentists and unscheduled visit required. Prolonged bleeding causing delayed discharge. Surgical bleeding – if judged by surgeon to be abnormal ie prolonged, delay in discharge, requires intervention. Menorrhagia – interferes with daily activities. Specific – change pads < 2hrly, > 7 days, clots > 1cm + flooding. PPH - > 6 weeks or considered significant by obstetrician. Muscle haematoma/haemarthrosis – significant if spontaneous CNS – significant Other – especially if occur in infancy