Download
1 / 33
330 likes | 581 Views
Direct Segment Optimization Optimizing conformal plans without IMRT. Jennifer M. Steers 1,2 , Martha M. Matuszak 1,2 , Benedick A. Fraass 1 Departments of Radiation Oncology 1 and Nuclear Engineering & Radiological Sciences 2 University of Michigan, Ann Arbor, Michigan. Outline.

E N D
Direct Segment Optimization Optimizing conformal plans without IMRT Jennifer M. Steers1,2 , Martha M. Matuszak1,2 , Benedick A. Fraass1 Departments of Radiation Oncology1 and Nuclear Engineering & Radiological Sciences2 University of Michigan, Ann Arbor, Michigan
Outline • Introduction • What is DSO? • Why are in we interested in DSO? • Goal • Methods and Materials • Results • IMRT vs. DSO comparisons • Conclusions
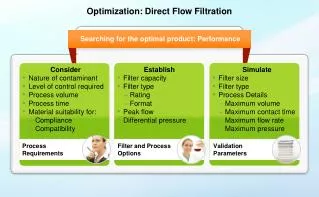
What is DSO? • Direct segment optimization (DSO) • form of direct aperture optimization (DAO) but based on flat fields, not on beamlet distribution • Utilizes user-defined cost functions to optimize the following: • Beam weights • MLC positions
Why are we interested in DSO? • Plans are optimized conformal plans • Can reduce delivery time over IMRT • Can result in fewer MUs when compared to IMRT • Plans do not require IMRT QA - plans could be started or adapted much quicker • It may make tweaking and optimizing leaf positions in conformal plans, such as SBRT, much quicker
Goal • Can DSO produce simpler plans comparable in quality to IMRT plans with the same beam angles and cost function?
Methods and Materials:Features of DSO • MLCs and beam weights can be optimized separately or together • Search strategy options • Ordered and random searches • Step sizes • DSO offers fewer degrees of freedom per beam when compared to IMRT • User must create segments in a plan before optimizing
IMRT vs. DSO Setup • Planning goal: Minimize dose to OARs and normal tissues without compromising target uniformity • Same gantry angles were used between the IMRT and DSO plans except when needed segments were added to the DSO case • The same cost function was used to optimize both the IMRT and DSO plans
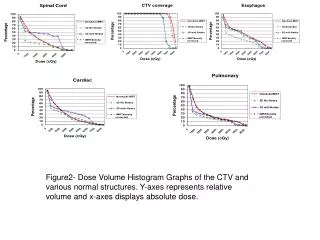
Evaluation of Comparisons • Both plans were optimized and evaluated with the following metrics • DVHs • MU/fx and beam-on time/fx • Mean doses to structures • Max structure doses (to 0.5cc or 0.1 cc) • D95 (for PTVs) • 3D dose comparisons
Brain Planning Goals • Target : 60 Gy (Min: 59, max: 61) • Normal brain: minimize dose (threshold 0, power 2) • Optic structures: minimize dose (threshold 0, power 2)
Normal Brain
PTV Normal Brain Chiasm
Plan Comparison Brain16 Brain11
IMRT vs. DSO 1x1 beamlet plan DSO plan Brain11
IMRT vs. DSO 1x1 beamlet plan DSO plan Brain11
Lung Planning Goals • Using adaptive protocol (2007-123) • PTV: 85 Gy (Min: 84 Gy, max: 86 Gy) • Esophagus: NTCP < 47% (Veff = 33%) • Heart: NTCP < 5% • Normal Lung: NTCP < 17.2% • All normal structures: minimize dose (threshold 0, power 2)
7-field, Non-coplanar Plan – Lung2-123
PTV Esophagus Heart Cord
PTV Esophagus Heart Cord
Plan ComparisonLung2-123 Lung2-123
PTV Normal Liver Cord
PTV Normal Liver Cord
PTV Normal Liver Cord
Plan Comparison Liver4 Liver4
IMRT vs. DSO 1x1 beamlet plan DSO plan Liver4
Conclusions • DSO can successfully optimize several types of planning scenarios while reducing treatment time • Optimizing with DSO can produce plans comparable in quality to IMRT with less MUs and segments • No need for the type of QA associated with IMRT plans • Overall plan complexity is less
Conclusions • In the future: • DSO may be more time efficient while yielding similar quality plans as IMRT in an adaptive re-planning scenario • Since DSO produces flat-field plans, it may be useful for cases with inter- and intra-fraction motion • Looking at other sites that could benefit from twiddling (prostate, SBRT, pediatric)