Download
1 / 83
910 likes | 1.37k Views
IMRT Commissioning. Gary A. Ezzell., Ph.D. Mayo Clinic Scottsdale. Welcome to Arizona. Commissioning elements. Validating the dosimetry system Commissioning the delivery system Commissioning the planning/delivery systems for dosimetric accuracy Learning how to use IMRT.

E N D
IMRT Commissioning Gary A. Ezzell., Ph.D. Mayo Clinic Scottsdale
Commissioning elements • Validating the dosimetry system • Commissioning the delivery system • Commissioning the planning/delivery systems for dosimetric accuracy • Learning how to use IMRT
Step 0: the dosimetry system • Decide on the system that will be used to measure dose distributions • Determine the measurement uncertainty • Compare measurements of unmodulated fields to ion chamber scans • Needed to establish acceptance criteria
Delivery system tests • Need to create test patterns independent of planning system • Need to check • MLC positioning accuracy • MLC dynamic motion accuracy • Effect of rounded leaf ends • MU linearity ...
Radiation field “offset” for rounded leaf ends • For rounded MLC leaf ends, there is an offset between the light and radiation field edges: ~0.6 mm • Important in IMRT Light Radiation
Measuring the offset • Irradiate a series of strips that abut • Use different values of offset • Select offset value that gives best uniformity
No offset 1.0 mm offset 0.6 mm offset Measuring the offset Here, 0.6 is best, i.e. subtract 0.6 mm from MLC settings Needed?? most uniform at junction? Integrated dose?
MLC accuracy • Tenths of millimeters are important for IMRT • Use patterns of abutting strips for a sensitive test • Test at different gantry and collimator angles • Select subset for routine QA
Abutments are very sensitive to positioning Offset 0.9 mm Offset 0.7 mm Offset 0.5 mm
DMLC tests • For dynamic MLC motion, leaf speed and dose rate also need to be controlled • Need to test for range of leaf speed and dose rates, as well as gantry and collimator angles • Create patterns that move a 1 cm gap using all leaves at same or variable rates
Sweep all leaves at same rate Chamber reading at center should be proportional to MU Film should show uniformity
Sweep leaves at different rates e.g. Travel 5, 7, 9, 11, 13 cm in same MU Check relative dose
Special problem of matching accelerators • In ’99 Mayo Clinic Scottsdale had two “matched” Varian 2100C linacs, but IMRT doses differed by ~2.5% • Needed to adjust MLC calibration on one machine by 0.13 mm
Delivery system QA • Sweep a 5mm gap across a 10 cm span with Farmer chamber at center • Take ratio to 10x10 open field • 2.5% for 0.2 mm change
Routine QA checks for positioning accuracy • Abutment films • 1 mm gap films • Check at different gantry, collimator angles • Check frequency(?)
Planning system: Dosimetric accuracy • For IMRT, the MLC leaves move through the area of interest • Final distribution is created by summing many beamlets • New things become important • Leakage through MLC leaves • Penumbra defined by MLC leaves • Small fields
MLC leakage - measure average value • Leakage through leaf (~2%) • Between neighboring leaves (~5%) • Measure using a pattern that fully closes all leaves - careful not to be under carriage or jaw
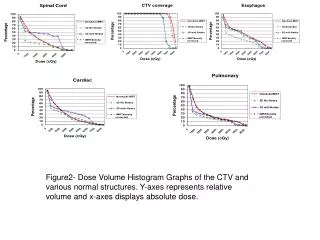
Penumbra • Measure with film, diode, or microchamber, conventional scanning chamber too wide • Subtle effects make a difference in IMRT Beam model based on penumbra measured with chamber Beam model based on penumbra measured with film
Dosimetric validation (1) Start with the basics • Define simple open fields irradiating a simple phantom • check calculated output, PDD, profiles against standard measurements • (just like commissioning any planning system) • And shaped static fields also
Dosimetric validation (2) • Define simply-modulated fields with wide regions that can be measured with chamber and film (or equivalent) • Check: • Leakage/transmission • Basic modulation • Penumbra • Out of field dose
100% centers, 10% wings 10% centers, 100% wings “Incline” patterns 50% centers, 100% -10% wings “Ridge” and “Trench” patterns Useful for deciding minimum segment width
“Band100” – “Band0” patterns 0% 60 20 10 80
What to do about differences? • May need to adjust the beam model • May need to live with it • That is, take known deficiencies into account when evaluating plans • Very important to know about it, especially for critical structures
Dosimetric validation (3) • Define targets and structures in a simple phantom: mock clinical situations • Create inverse plan • Measure doses with chamber, film, … • Evaluate dose/MU in low gradient region • Evaluate isodoses on many planes
Dosimetric evaluation of mock clinical plans • What kind of agreement to expect in high dose, low gradient regions? • ~2 - 4% is reasonable (chamber) • What kind of agreement to expect for isodoses? • Much harder to specify • ~2 - 4 mm for 50% - 90% lines
How to be more quantitative? • Acceptance criteria should be stated statistically, such as: “within the region of interest, 95% of the calculation points should agree with the measurement to within 5%,which combines the desired degree of agreement with reality (3%)with the two-sigma uncertainty in the measurement technique (4%).”
Questions • What is the region of interest? • What is the desired degree of agreement with reality? • What is the uncertainty in the measurement technique? • What percentage of the points should agree to the specified tolerance?
Questions • For the points that do not agree to that tolerance, is there an outer limit of acceptability? • Should the agreement be expressed as a percent of the local dose, prescription dose, or some other dose? • Should distance to agreement be incorporated?