Download
1 / 25
250 likes | 492 Views
Mount Vernon Cancer Network. Skin Cancer. Dr Veronique Bataille, MD PhD FRCP Consultant Dermatologist West Herts Hospitals NHS Trust Hemel Hempstead Hospital. Skin cancer statistics. Melanoma. The most dangerous form of skin cancer affect around 16/100.000 in the UK

E N D
Mount Vernon Cancer Network Skin Cancer Dr Veronique Bataille, MD PhD FRCP Consultant Dermatologist West Herts Hospitals NHS Trust Hemel Hempstead Hospital
Skin cancer statistics Melanoma. The most dangerous form of skin cancer affect around 16/100.000 in the UK Mortality is much lower than incidence as most melanoma patients now survive: nearly 90% at 5 years now in the UK However, this is highly correlated with early detection as late presentation fares badly The mean age is 50 years and melanoma does not occur in sites most exposed to sunlight unlike the other types of skin cancers
Skin cancer and risk factors For melanoma: high number of moles, family history of melanoma, fair skin with freckles, strong family of cancer For SCCs: chronic sun exposure over a lifetime, fair skin, immunosuppresion For BCCs: Sun exposure below 20 years, fair skin, family history of BCC SKIN CANCER IS VERY RARE IN NON-CAUCASIANS so think other diagnoses
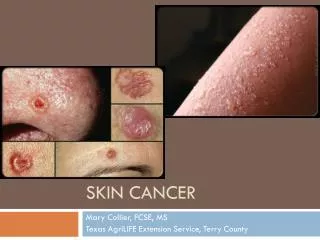
Squamous cell carcinoma SCC/BCC is ratio is ½ The exact incidence is now as clear as melanoma as SCCs are poorly registered These tumours occur in the elderly and on the most sun exposed sites such as face/hands/arms The mean age is in the 70s They are very rarely lethal although high risk sites are lips, fingers and genitals.
Keratoacnathoma “Benign” squamous proliferation of the epithelium Grow fast over weeks Big shoulder Central crusting If left alone involute But most get removed—differential diagnosis with SCC Syndrome of mutliple keratoacanthomas: Ferguson Smith
Basal cell carcinoma The most common form of skin cancer Not lethal Affect sun exposed sites although young individuals are more prone to trunkal lesions Mean age 60s Grows in months rather than weeks Different subtypes: nodular/cystic, superficial, infiltrative/morphoeic and pigmented.
Melanoma statistics locally • Incidence • MM UK wide in 2009: 16/100.000 • Hertfordshire 2009: 17/100.000 • Luton 2009 9/100.000 • Survival • 3 years UK: 92% • 3 years Herts:92% • Luton: 83.5%
Survival at 5 years • UK 88.4% • Herts 97% • Luton 87% So it appears that the Luton area does far worse. This may be due to several factors. Higher socio-economic groups may have more screening hence thinner lesions and also possible difference in reporting by pathologists However, it could also be due to genuine delay in diagnosis
2 ww • Should be used ONLY for suspected MM and SCC • Important signs: new pigmented lesion growing, existing lesion changing, asymetry in colour and border for MM • SCC: red nodule often with crusty top., growing in matter of weeks or months, sun exposed sites, elderly • Very slow growing lesions which are skin coloured are likely to be BCC and should not be referred via the 2 ww • Melanoma is extremely rare in children and children acquire new moles so the rules should be adapted to the age group
Conclusion • 2 ww form a large part of our workload • Important to select the right patient for this service • 1600 referrals at West Herts in 2011 • Most skin lesions do not need the 2 ww referral route • Melanoma and SCC behave differently from BCC and solar keratoses • Asymetry in colour and shape is important for melanoma. Recent changes in weeks or months • For SCC, there are often nodular and crusty and grow much faster than BCC