Download
1 / 131
1.48k likes | 2.03k Views
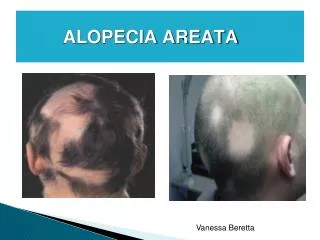
Scarring Alopecia. Dr Amir Hossein Siadat M.D. Alopecia. None Scaring (Reversible). Scaring (Irreversible). The term cicatricial or scarring alopecia : potential of permanent destruction of the hair follicle. Clinically: there is effacement of follicular orifices.

E N D
Scarring Alopecia Dr Amir Hossein Siadat M.D.
Alopecia None Scaring (Reversible) Scaring (Irreversible)
The term cicatricial or scarring alopecia : potential of permanent destruction of the hair follicle. Clinically: there is effacement of follicular orifices
Dissecting Cellulites: • Synonyms: • dissecting folliculitis • dissecting perifolliculitis. • most commonly begin on the vertex or occiput
Presents as relatively painless, deep-seated, firm to fluctuant nodules and abscesses.
The nodules and deep abscesses commonly extend to form: a complex serpiginous or reticulate pattern of interconnecting sinuses and abscesses filled with purulent, seropurulent, or hemopurulent material.
Pressure applied to one nodule or abscess: can cause purulent exudate to emerge several centimeters away. • The epidermal surface overlying the sinuses and nodules may or may not be erythematous and scaly. • Scattered superficial follicular pustules are frequently present on the surface of the nodules. • Hypertrophic and keloidal scarring may occur in affected areas.
Dissecting cellulitis of the scalp: more common in young to middle-aged black men. • It may occur simultaneously with acne conglobata and hidradenitissuppurativa. This complex is known as the follicular occlusion triad.
Pathology of Dissecting Cellulities • Biopsy specimens from well-developed fluctuant nodules and sinuses reveal large, perifollicular, mid to deep reticular dermal abscesses often rich in plasma cells. • Abscesses are located immediately adjacent to follicles, between follicles in the mid and deep reticular dermis, and subjacent to follicles within the superficial subcutis.
culture of abscess fluid and overlying pustules: frequently sterile may yield Staphylococcus epidermidis or S. aureus. • The pathogenic role of these organisms is uncertain because chronic antibiotic therapy is frequently not curative.
Treatment of Dissecting Cellulities • Initial therapy : oral antibiotics tetracycline (1 -2 g per day), doxycycline (200 mg per day), and minocycline (50-200 mg per day). • Combination antibiotic therapy of cephalexin (1 g per day) and rifampin (600 mg per day) has been helpful.
Intralesional corticosteroid injections (triamcinoloneacetonide, 40 mg/mL) can be helpful in noninfectious nodules and sinuses. • Oral corticosteroids tapered to low-dose alternate-day usage may also be helpful. • Isotretinoin (1 mg/kg per day) has been effective in some reported cases.
Oral zinc has also been reported to be effective. • Surgical therapy may be considered in advanced cases but is usually quite deforming. • Complete scalp excision, carbon dioxide laser excision, or more conservative local incision and drainage of individual lesions maybe considered.
destructive pustulofollicular process • occurs on the occipital scalp and posterior neck • primarily affects young black men.
begin as discrete follicular pustules and papules • progress to form less discrete, large, exophytickeloidal nodules and plaques largely devoid of hair.
The severity : few small follicular pustules and papules with minimal alopecia extensive keloidal plaque formation with prominent patterned alopecia Similar lesions may occur in the beard area of patients with pseudofolliculitisbarbae.
Pathogenesis and Etiology • The etiology : unknown • acne keloidalisnuchae : a variant of acne vulgaris • Bacteria may be isolated.
Repetitive low-grade trauma • friction by football helmets, other headware, and collars • Closed shaving of posterior scalp and neck hair
Treatment of Acne Keloidalis Nuchae Tetracycline, 1 g per day • Doxycycline 200mg/day • Minocycline 50-100mg/day • Erythromycin 1g per day • 2. Topical antibiotics. • Erythromycin solution 2% • Clindamycin solution 1% • 3. Tretinoin cream or gel 0.025%-0.1% • 4. Benzoyl peroxide gel or lotion 5%-10% • 5. Intralesional corticosteroid injections (triamcinolone acetonide, 3-40 mg/mL) • 6. Surgical excision for large exophytic keloidal
Discoid Lupus Erythematosus • Discoid lupus erythematosus is a common lesion • typically found in young to middle-aged adults • 2:1 female/male predominance. • Age at onset : between 20-60 years
most commonly located on the face, scalp, and inner ear 50% of patients with DLE have scalp lesions 10% of patients: only scalp involvement
Patients with discoid lupus: uncommonly progress to involvement with systemic lupus erythematosus. 15% of patients with SLE may exhibit DLE
Early lesions: small erythematous papules or irregular small, scaly plaques round to irregular shaped atrophic, sclerotic plaques.
Thick,adherent scale frequently develops that when removed reveals keratinous plugs on its undersurface.
When DLE is active: surrounding borders erythematous and violaceous. symptomatic including pruritus, burning and pain. • Both hyperpigmentation and hypopigmentation is frequently seen.