Download

1 / 22
220 likes | 321 Views
Recent Changes and Controversies. 4th Edition - Minimising Airborne Contamination. B2.1 “ there shall be a designated inpatient unit that minimises airborne microbial contamination B2.2 “ designated outpatient area......” Standards now recognise

E N D
4th Edition - Minimising Airborne Contamination B2.1 “ there shall be a designated inpatient unit that minimises airborne microbial contamination B2.2 “ designated outpatient area......” Standards now recognise • Variation in unit facilities – number, case mix, prevalence of opportunistic infections • Increased use of ambulatory approaches with frequent day case review • Do not imply that all units must have LAF • Important to provide data on effectiveness of approaches used
4th Edition - Admission to Intensive Care • B2.1.1 “The in-patient program shall have an intensive care unit or equivalent coverage within the institution” • B2.2.1 “Outpatients shall have a plan for providing immediate access.....” • Covers both inpatient programmes and outpatient facilities • Arrangements must be documented • IP within the facility; OP not necessarily on-site
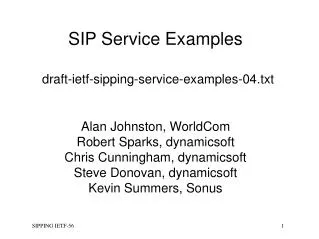
TBI conditioning ATG HSC infusion NK T CD8+, B T CD4+ d-7 0 months 6 9 1 3 12 isolation MTX/CsA GVH prevention Acute GVH treatment 0 2 1 3 months 5 4 HSV CMCCMV, EBV, adenovirus, VZV Main Opportunistic infections Candida aspergillus bacteria Discharge - Period of Time Covered by Standards?
Planned Discharge to Referral Centre • B2.3.5 “Planned discharge shall be to facilities adequate for post-transplant care. The CP is responsible for ensuring that the receiving centre provides care that meets applicable standards” • What is the limit for this – d30 auto; d100 allo ? • Responsibility of the TC to ensure compliance with items such as - Isolation facilities • Staffing and training • Policies and procedures • JACIE will require documentation of compliance and may include inspection of the hospital providing post-transplant care
Outpatient Facilities • B2.3 “There shall be a designated area for outpatients.....” protect from infections and allow appropriate isolation, administration of IV fluids, medications and/or blood products • Deficits include lack of space to allow proper segregation of patients with significant infections
4th Edition - Collection Facility Director • C3.2.1 “there shall be a collection facility director who is an individual with a medical degree or a degree in a relevant science” - requirement for a PhD dropped - Allows more nurses to become CFD - Emphasis also on postgraduate training and experience
4th Edition - Collection Facility Other changes • Donor section harmonised with B6 • Labels – clear legible and use ink that’s indelible to all relevant agents • Labels – also include concurrent plasma and samples – assigned the same identifier • Biohazard, warning and completion of collection labels – all info removed to table at Appendix 1. • C7.8 Accompanying docs at end of collection applies only to products collected in the USA or designated for use in the USA e.g. statements of ‘donor eligibility’
ABO testing and Compatibility • B6.3 “allogeneic CTPs; a test for ABO group and Rh type shall be performed on the first product collected or on blood obtained from the donor at the time of first collection” • Testing requirement for allogeneic donors on each and auto donors on 1st day of collection removed • Guidance: (i) document donor and recipient ABO/Rh prior to collection (ii) SOPs to manage ABO mismatch should be established
4th Edition - What is a Clinical Programme? • Clinical Standards cover cell therapy at present mainly HSCT, C and D refer to cellular therapy • B1.1 “ an integrated medical team housed in geographically contiguous or proximate space with clinical programme director(s) and common staff training programmes, protocols and QMS” • Non-contiguous sites must be in defined networks - community programme with 2 hospitals in the same area - NHS Trust in the UK - Cancer networks - other robust structures involving centres/satellites • Units should be , 1 hour travelling time
Areas of deficienciesExpressed as % of total deficiencies. Based on analysis of 1732 deficiencies encountered in inspections
Minor v Significant Deficiencies • Difference between a minor deficiency and a significant deficiency is a matter of judgement • Minor deficiencies • generally involve correction to existing SOPs or other documentation • Significant deficiencies - examples • Inpatient isolation facilities inadequate • No continuous temperature monitoring of freezers • Inadequate quality management programme
Interactions Between Facilities • Collection facility must use processing facilities that meet JACIE standards • Bone marrow collection normally integral to clinical programme but must be inspected and accredited as a collection facility • Apheresis collection and processing facilities may be integral to programme, or external, e.g. National Transfusion Service
Interactions Between Facilities Links between facilities are important e.g. • Written requests for collection, or component issue • Provision of engraftment data to collection and processing facilities • Reporting of AE’s to other facilities, if appropriate • Service agreements or contracts with external facilities
At the end of the inspection The exit interview • Inspector should discuss any sensitive issues with facility head and/or Programme Director in private BEFORE exit interview • The inspectors discuss their visit and inform the Programme Director and staff of what they found • Inspectors do not comment on possible outcome • Inspectors should not express personal opinions about standards
Reporting after the Inspection • Complete checklists with reasons where required • List key personnel • Short report summarising structure and operation of collection facility • Send to team leader promptly!!
Inspection report Corresponds with the exit interview i.e. no surprises
The Inspector Inspectors return Completed Inspection Checklist, any notes and documents to the Team Leader (TL) or directly to JACIE Office TL compiles summary inspection report based on discussions with the other inspectors and their observations
Confidentialty • Inspectors should not discuss inspection with colleagues • Return any documents or notes to Team Leader or JACIE Office • Inspector can ask centre for permission to use and SOPs, labels etc. • Applicant centre is entitled to refuse
Summary • Be aware of new standards • Read documentation thoroughly before visit • Decide who to speak to on the day and on points to clarify • Ask members of collection facility staff to show you what they do • Be interested, kind, supportive and patient!!