Download
1 / 51
730 likes | 1.32k Views
Calcified Coronary Lesion: Difficulties and Challenges. Zhou Yu Jie MD, PhD, FACC, FSCAI, FHRS Beijing An Zhen Hospital, Capital Medical University, Beijing, China. Sweet dream or nightmare ?. Marker for CAD and increased mortality. 4,609 asymptomatic individuals

E N D
Calcified Coronary Lesion:Difficulties and Challenges Zhou Yu Jie MD, PhD, FACC, FSCAI, FHRS Beijing An Zhen Hospital, Capital Medical University, Beijing, China
Marker for CAD and increased mortality • 4,609 asymptomatic individuals • Follow-up 3.1 years • 4,425 Suspected CAD patients • Follow-up 3 years JACC: CARDIOVASCULAR IMAGING. 2010 Dec;3(12). JACC: CARDIOVASCULAR IMAGING. 2012 Oct;5(10)
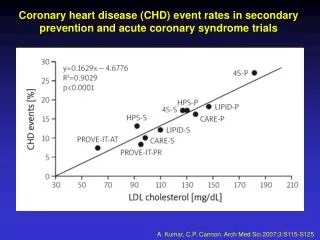
Coronary Artery Calcium (CAC) in the Multi-Ethnic Study CAC are associated with CHD events Coylewright et al. Atherosclerosis.2011
Risk Factors(The MESA study) • Race and gender • Age • BMI • Smoking • Family history of heart attack • Hyperlipidemia Intimal calcification • Hypertension Intimal calcification • Diabetes Medial calcification • CKD Medial calcification • Rheumatic diseases Circulation. 2007;115:2722-2730
Inverse relationship between BMI and CAC Atherosclerosis. 2012 March ; 221(1): 176–182. Method: • 9,993 patients undergoing PCI • The degree of index lesion calcification (ILC) based on angiography
Elevated BSA is a predictor of CAC, not BMI Method:3172 consecutive patients underwent CAC scores Coron Artery Dis 2012 Mar;23(2):113-7
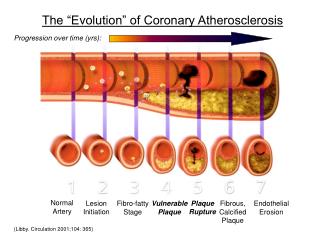
Mechanism of CAC Vascular calcification is an active ,regulated process BMP-Smadsignaling BMP-Wnt signaling
Major Theories of Vascular Calcification DISTURBED Ca/Pi BALANCE Hyperphosphatemia Hypercalcemia DISTURBED Ca/Pi BALANCE Hyperphosphatemia Hypercalcemia DISTURBED Ca/Pi BALANCE Hyperphosphatemia Hypercalcemia DISTURBED Ca/Pi BALANCE Hyperphosphatemia Hypercalcemia DISTURBED Ca/Pi BALANCE Hyperphosphatemia Hypercalcemia DISTURBED Ca/Pi BALANCE Hyperphosphatemia Hypercalcemia INDUCING FACTORS Pi Lipids Inflammatory cytokines Others INDUCING FACTORS Pi Lipids Inflammatory cytokines Others INDUCING FACTORS Pi Lipids Inflammatory cytokines Others INDUCING FACTORS Pi Lipids Inflammatory cytokines Others INDUCING FACTORS Pi Lipids Inflammatory cytokines Others INDUCING FACTORS Pi Lipids Inflammatory cytokines Others LOSS OF INHIBITION Pyrophosphate MGP OPN Fetuin/alpha2-HS glycoprotein Others Ca x Pi INDUCTION OF BONE FORMATION Vascular bone and cartilage-like cells INDUCTION OF BONE FORMATION Vascular bone and cartilage-like cells INDUCTION OF BONE FORMATION Vascular bone and cartilage-like cells Vascular calcification INDUCTION OF BONE FORMATION Vascular bone and cartilage-like cells INDUCTION OF BONE FORMATION Vascular bone and cartilage-like cells CIRCULATING NUCLEATIONAL COMPLEXES CIRCULATING NUCLEATIONAL COMPLEXES CIRCULATING NUCLEATIONAL COMPLEXES Matrix Vesicles Matrix Vesicles Matrix Vesicles Matrix Vesicles Matrix Vesicles Apoptotic bodies Apoptotic bodies Apoptotic bodies Apoptotic bodies Apoptotic bodies Bisphosphonates OPG Bisphosphonates OPG Bisphosphonates OPG Bisphosphonates OPG Bone Remodeling Bone Remodeling CELL DEATH CELL DEATH CELL DEATH CELL DEATH
No effective medicine treatment • Evidence from meta-analyses Statin and LDL-C Statin and calcification Coylewright et al. Atherosclerosis.2011
Statins promote CAC (VADT trail) Saremi et al. Diabetes Care.2012;2390-2
Strategy of PCI in CAC • Balloon angioplasty • Cutting balloon • Rotablator • Stent • Post dilation • Laser
Strategy for balloon angioplasty • Small size balloon prefered • Pressure of BC from 8 atm, slowly increase • The up limit of pressure may be 16 atm • Flow restricting dissection or perforation be concerned 14
Cutting balloon for calcified lesion • Indication for cutting balloon: Lesion relatively short (<20mm) Concentric lesions • Heavily calcified lesion not appropriate, but sometimes brought supprise 15
Rotablator for calcified lesion • Effective device for calcified lesion • Differential tissue cutting ----selectively hard lesion, no soft tissue • Optimal burr size---60%-70% of reference vessel diameter • Prevent no flow & slow flow ----nitroprusside, adenosine , etc • Upper limit of rotablator: just enough for revascularization 16
Rotational Atherectomy(RA) RandomizedROTAXUS Trial Outcome JACC Cardiovasc Interv 2013 Jan;6(1):10-9
Randomized ROTAXUS Trial Outcome CONCLUSIONS: • RA does not increase the efficacy of DES in calcified lesions • Using RA did not reduce late lumen loss of DES at 9 months • RA remains the default strategy for complex calcified lesions Death MI TVR MACE JACC Cardiovasc Interv 2013 Jan
Analysis of the UK central cardiac audit database Method: • 221,669 PCI procedures • 2152 patients (0.97%):RA (RA+) • Remainder conventional PCI: (RA-) CONCLUSIONS: • RA was undertaken in patients with higher pre-procedural risk. • Medium term survival was worse among patients undergoing RA. • Procedural success and complication rates seem acceptable in this context. RA remains clinically useful for patients with calcified coronary lesions. Int J Cardiol. 2014 Jan 1;170(3):381-7
Rotational atherectomy for LM in octogenarians • 42 patients ≥80 years had undergone stenting for calcified LMCA disease • Procedural successis good (92.3% vs. 96.6%) • RA appeared to be a safe and effective strategy for the treatment of LMCA disease in octogenarians who were refused for surgery Int J Cardiol 2013 Apr;26(2):173-82
Rotablator for failed angioplasty • An 84 year man • Previous failed angioplasty due to balloon rupture • CAG showing severe CCL 21
23 Stent deployment
Rotational Atherectomy and IVUS Pre Pre Post RA 1.75 mm burr b a Post 1.75 mm burr RA
DES for calcified lesion • DES use was associated with a significantly lower risk in repeat revascularization (HR = 0.57; 95% CI 0.40–0.82; P = 0.002) compared to BMS group in CCL • TAXUS-IV sub study : 9-month angiographic follow-up, DES significantly reduced the amount of late loss compared with the BMS (0.26 +/- 0.56 vs 0.51 +/- 0.48 mm, p = 0.015) in the calcific lesions 25 Sripal Bangalore, CCI 77:22–28 (2011) Moussa I, Am J Cardiol. 2005 Nov 1;96(9):1242-7
Post dilation for calified lesion • Post dialation last straw for calified lesion • Non compliant, high pressure balloon first choice • Be careful coronary perforation or serious dissection 26
Progressive deterioration of chest pain for 3 years (CCS II), presented with unstable episodes in last 2 weeks (CCS III) With a history of HBP, prior inferior and anterior myocardial infarction 2 1 Clinical presentation Male, 84-year-old Diagnosis: UAP Prior MI Hypertension 3
Laboratory tests • TnI levels of 0.01 ng/mL (normal range, <0.05 ng/mL), Cre 76umol/L, ALT 23U/L, AST 34U/L • A 2-dimensional echocardiogram demonstrated decreased left ventricular function, with an ejection fraction of 41%
The patient refused the surgical solution and medical conservative therapy After discussion the decision was made to perform sequential PCI: RCA CTO first, then unprotected LM lesions Treatment strategy
PCI for RCA GC: JR 4.0, GW: Pilot 50 Predilation BC: Sprinter 1.5 x 15mm and 2.0 x20mm
Final result-RCA DES implantation: Firebird2 2.75x33mm for d-RCA and Partner 3.0x36mm for p-RCA
PCI for LM 1 week later GC: EBU 3.5, GW: BMW (to LAD) and Runthrough NS (to LCX)
PCI for LM-Predilation Predilation BC: Sprinter 2.5 x 15mm, 12-20atm
PCI for LM-1st Stent Implantation DES implantation : Firebird2 2.75x23mm for m-LAD (12atm)
PCI for LM-2nd Stent Migration LM/p-LAD Stent Migration (Cypher 3.5x33mm), exchange to 8F sheath
PCI for LM-Retrieving Stent Migrated stent was retrieved successfully assisted with Sprinter 1.5x15mm
PCI for LM -Continue with Mini-Crush Continue with 7F EBU 3.5; Mini-Crush technique was used Firebird2 3.5x33mm for LM/p-LAD and Firebird2 3.0x18mm for LCX
PCI for LM-Postdilation Postdilatation with Avita HP 3.5x15mm (14-20atm for LM/p-LAD stent)
PCI for LM-1stFinal Kissing 1st final kissing with Avita HP 3.5x15mm (LAD) and Sprinter 3.0x12mm (LCX)
2nd IVUS test LAD ostia stent expansion unacceptable
PCI for LM-Re-postdilatation Re-postdilatation with Avita HP 3.5x15mm (18-24atm for LM/p-LAD stent)
PCI for LM-2stFinal Kissing 2nd final kissing Avita HP3.5x15mm (LAD) and Sprinter3.0x12mm (LCX)