Download
1 / 34
350 likes | 604 Views
Electrolyte Disorders. Dom Colao, DO November 2011. Review of Electrolyte disorders. HypoNatremia Hypernatremia HypoKalemia HyperKalemia Calcium Magnesium Phosphorus. Overview of Disorders. The differential for any lab abnormality: Lab error Lab error Lab error Polypharmacy

E N D
Electrolyte Disorders Dom Colao, DO November 2011
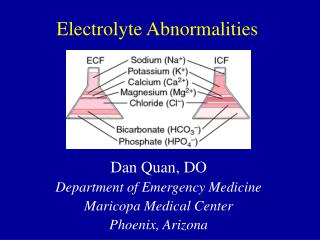
Review of Electrolyte disorders • HypoNatremia • Hypernatremia • HypoKalemia • HyperKalemia • Calcium • Magnesium • Phosphorus
Overview of Disorders • The differential for any lab abnormality: • Lab error • Lab error • Lab error • Polypharmacy • Iatrogenic • Real disease • In that order!
Always consider the potential for a confounding variable • Was the blood drawn above a running IV? • Did it sit too long before the test was run? • Is it your patients blood? • Is there a pattern of abnormalities in numerous patients on the same day?
Over view of Sodium Disorders • Pseudo-hyponatremia • Due to high concentrations of other solutes in the blood - Mannitol in a pt with cerebral edema, Glucose in a diabetic. • Then look at the patient’s volume status • Hypervolemic/Euvolemic/Hypovolemic
Hyponatremia • Hypervolemic: • HypOvolemic: • Euvolemic:
Hyponatremia • Hypervolemic: • CHF, • Cirrhosis, • Pregnancy, • Nephrotic syndrome • In these conditions, total body sodium is up, but total body WATER is up even more. • Due to reduced Effective Arterial Blood Volume, (EABV) leading to increased ADH secretion.
Hyponatremia • Hypervolemic: • CHF, Cirrhosis, Pregnancy, Nephrotic syndrome • HypOvolemic: • GI losses (diarrhea, Vomiting, NG suction) • Renal Losses (diuretics, Salt wasting nephropathy, recovery phase from ATN or obstruction). • Due to true depletion of water and sodium, leading to increased secretion of Aldosterone AND ADH
Hyponatremia • Hypervolemic: • CHF, Cirrhosis, Pregnancy, Nephrotic syndrome • HypOvolemic: • GI losses (diarrhea, Vomiting, NG suction) • Renal Losses (diuretics, Salt wasting nephropathy, recovery phase from ATN or obstruction). • Euvolemic: • Medication effects, Endocrine syndromes, Excessive water intake, reset osmostat, SIADH
Hyponatremia • Euvolemic: • Medication effects • ACE/ ARB/Tekturna/Spironolactone/HCTZ • Antidepressant and antipsychotic meds • NSAID’s • Endocrine syndromes • Hyper and Hypo thyroid, • Adrenal insufficiency and excess (addison’s / Cushings) • Excessive water intake, • Psychogenic polydipsia, beer potomania • reset osmostat, • Seen in conditions which stimulate tonic ADH secretion from tissues which have Neuroectoderm (brain and Lung) • SIADH
Hyponatremia • Euvolemic: • reset osmostat, • Seen in conditions which stimulate tonic ADH secretion from tissues which have Neuroectoderm (brain and Lung) • Pneumonia, COPD, stroke, brain hemorrhage. • These conditions result in a stable low level of sodium, around which water and sodium regulation are functioning normally, but at a new lower setting. • Confirmed by water loading test. • SIADH - Persistant high production of ADH which does not suppress in the face of water load, usually due to a tumor such as small cell lung carcinoma or brain tumor.
Case 8 Hypermagnesemia • Hypermagnesemia is seen only in patients with renal failure who are supplemented, • or in cases where large amounts of magnesium are infused.
Case 9 Hyperphosphatemia • Classic presentation of Hypophosphatemic rhabdomyolysis. • Prolonged NPO status/starvation • Resp failure requiring reintubation after extubation or surgery. Due to resp muscle weakness. • Phos goes very low, then suddenly climbs without any supplementation. Associated with high K and Low calcium. • Creatinine climbs more than 1.0 mg/dl/day, suggesting increased creatinine production
Reference • Narins. Fluid and Electrolyte Disorders: Am journal of Medicine, 1982