Download
1 / 50
510 likes | 727 Views
House of Lords. The Roscoe Lecture Cancer, care and compassion Ilora Finlay of Llandaff. “How people die remains in the memory of those who live on.” Cicely Saunders. Compassion Moral courage Antislavery voted against it during brief time as an MP. William Roscoe Compassion

E N D
House of Lords The Roscoe LectureCancer, care and compassionIlora Finlay of Llandaff “How people die remains in the memory of those who live on.” Cicely Saunders
Compassion Moral courage Antislavery voted against it during brief time as an MP William Roscoe Compassion Moral courage Antislavery voted against it during brief time as an MP WilliamRoscoe
End of life care – a political issue • 500,000 deaths per annum in UK • 2/3 over 75 years • 1/3 over 85 years • Predict by 2030, will rise to 44% over 85 years (Gomez, Higginson) • £££ • Baby boomers • Always ‘had it good’ • High expectations • Controllers • Voters
Kitty Wilkinson's story is one of unbelievable determination, courage and selflessness. Saint of the slums
Some public concerns • Symptoms • Died in agony • Growing numbers elderly • Demographic time bomb • Children and adolescents • ‘Assisted dying’ • Society for Old Age Rational Suicide • Living wills • Advance decisions
Emotional Total Pain Social Spiritual Physical
Diagnosis is key Symptom Diagnosis Prescribing No relief Relief
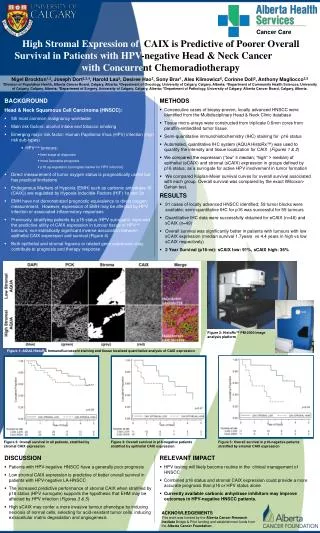
Life prolonging palliative care • Temel JS et al NEJM 2010;363:733-42 • Early palliative care for patients with metastatic non-small-cell lung cancer • Quality of life • Mood • Survival (11.6 v 8.9 months, p=0.02)
Integrated care? Grief Curative intent Palliative Care Physical Social Spiritual Emotional
‘The quality of life gap’ not a magic bullet Hopes and aspirations Gap Reality Time K Calman
Care at the end of life Diagnose irreversibly dying Check all futile medication ceased Consider fluids for comfort Plan for what might be needed Keep comfortable / keep checking Make sure family informed and aware
Involving palliative care at time of need • deteriorating • Bereavement • Palliative Care Outcomes Collaborative Assessment tool definitions: Phase V 1.2 December 2008
Dignityis havinga sense of personal worth Dame Cicely Saunders 1992
Dignity “Care that confers honour, recognised the deservedness of respect and esteem of every individual - despite their dependency, infirmity and fragility - could lie at the heart of care that conserves dignity” Chochinov H et al Lancet 2002
Dignity Intrinsic dignity Relational dignity Attributed dignityperson/society Experienced dignity Courtesy of Carlo Leget Univ of Tilburg
Nothing about me without me Choice Control
Wales policy Board 2008-117 day service • 24/7 unaffordable • Compromise: • All CNS (band 7/8) contribute to 7 day working • Consultant cover for whole of Wales • Agenda for Change - £140,000 • Partnership working
The children as relatives and carers • Fragmented families • Grandparent can provide: • Security • Unconditional love • Guidance, wisdom • Confidante
Children 5-16yr 7,000 / m death of a parent or sibling 13,000 / m bereaved of a friend Plus children in care Bereavement care is the most effective form of preventative medicine Remember the children
A common story? • 84 years old • Advanced cancer • Pain on any movement • In hospice • I’ve had a good life – I’ve had my time • I just want to die!
I just want to die Courtesy of Irene Higginson
Fear the future worse than today Pain Loss of dignity (mind / body) Loss of control Loss of autonomy Being a burden
How we all make decisions Experience Memories Formal info. Media Feelings Non-verbal cues 90% communication Reactions
Who steers the consultation? I just want to die!
So you really want to die? Listen Process request Message = you are right to think that you’d be better off dead What is making today so terrible? What can we do to improve today? Message = you are worth me working hard to improve things
Autonomy is relationalOur living and our dying have an effect on those around us
Ending suffering? End life
Compassion • Would the compassionate response be to end life by assisted suicide / euthanasia? • Why not change the law?
The law on medical decision-making • Mental capacity act • Best interest decision • Advance decisions to refuse treatment • Advance statement of wishes • DPP guidelines on prosecuting assisting suicide • Compassion • Not part of care-taker role
But what about safeguards? • Part of healthcare • Terminal illness • Mental capacity • Freedom from coercion • Fully informed • Cooling off period • Self administration • Immunity in advance
Trust of the doctor (or pilot) • Patients have to trust doctors to give advice & treatment in best interests • Trust makes patients particularly vulnerable • Society ‘comforted’ by trust of doctor
Doctor’s duty to relieve suffering • Unbearable versus unrelievable suffering • Existential suffering
Ending suffering? Intervene time Capacity to experience = personhood
Just the ‘terminally ill’ • Incurable illness • Prognosis <6 months • “medicine is a probabilistic art” • Diagnostic errors – 5% at post-mortem • Prognosis notoriously inaccurate • When defined as in ‘last 48 hours of life’, 3% improve again
Oregon <6 months prognosis N= Request to death 15 – 1009 days [2 yr 9 mos]
Informed choice and decisions • Cognitively demanding – ‘compos mentis’ • MND 30% cognitively impaired (HoL) • 1 in 8 PAS in Oregon had Motor Neuron Disease • Depression • Oregon study 18 patients prescription for PAS • 9 died PAS • 3 had undiagnosed /untreated depression • “the current practice of the Death with Dignity Act may not adequately protect all mentally ill patients” Ganzini2008 BMJ
Truly voluntary decisions? • Pressures - internal or external • Fluctuant desire for PAS • “Compassion” Loved ones • Influence of physician • Normalisation in society becomes expectation
Careful assessment? • Oregon: • 1 dr. wrote 11 prescriptions last year • Campaign group act as ‘broker’, ‘guardians of the law’ • Fall in psychiatric referrals to zero • No audit of content of assessments • No prescription monitoring • In Belgium anonymous survey reveals almost half euthanasias are outside their law
Timing • Cooling off – for how long? 2 weeks? • Prior licence
Autumn 1991 39 36 12 8 6/52
1991 Spinal tumour Becoming paraplegic Clear thinking Adamant – euthanasia GP: ‘I’m only referring him because I cannot give him a lethal injection’
2002 • Telephone call from him • Wife admitted hospice died 18 days later • He was in wheelchair • Children present, fully aware
Law framed for a very few highly resolute strong-minded individuals? In an ideal world of wholly autonomous patients, wholly selfless & compassionate families & professionals …… it might be safe But we do not live in that world… ‘we should not put too much weight on the fragile structure of the voluntary’ Onora O’Neill 2010
Not a medical care duty Euthanasia Physician assisted suicide Assisted suicide
4 years after wanting death • I am ….. at the end of my life, in bed & unable to do, but able to receive and find an unexpected serenity in receiving. • A week ago my wish to die resurfaced; yet my ability to live resurfaced too.