Download
1 / 107
1.13k likes | 1.37k Views
Fetal circulation. Dr Sreejith a g Senior resident,dept.of cardiology. Fetal circulation. First functional system of embryo at 21 days Most of the work has been done in fetal lambs. history. First recorded mention of fetal circulation-Galen

E N D
Fetal circulation Dr Sreejith a g Senior resident,dept.of cardiology
Fetal circulation • First functional system of embryo at 21 days • Most of the work has been done in fetal lambs
history • First recorded mention of fetal circulation-Galen • W.harvey- (1628)-ventricles in fetus work in parallel • Dawes –changes in circulation at birth • Rudolph-fetal circulation in lambs
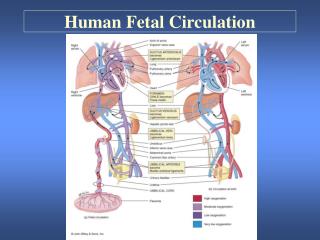
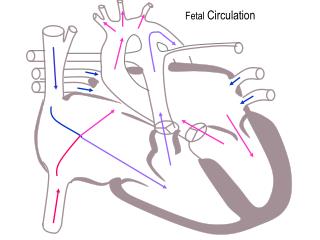
Fetal circulation • Central circulation Arteries Veins Shunts • Peripheral components Various regional vascular beds
Salient features • Placenta is the site of gas exchange • Presence of shunts • Parallel arrangement of two main arterial systems and their respective ventricles. • Preferential streaming of blood • High impedance and low flow of pulmonary circulation. • Low impedance and high flow of placental circulation.
The pressures in right system is higher • Fetal myocardial energy requirements are met by lactate • Concentration of Hb in fetal blood is about 50% more than mother
Shunts in the fetal circulation The fetal circulation is characterised by four shunts. • first, within the placenta • second, across the ductus venosus • third, through the foramen ovale • fourth, across the ductus arteriosus
The Placenta • Facilitates gas and nutrient exchange between maternal and fetal blood. • The blood itself does not mix.
Umbilical Circulation • Pair of umbilical arteries carry deoxygenated blood & wastes to placenta. • Umbilical vein carries oxygenated blood and nutrients from the placenta.
Oxygen exchange function • Higher hemoglobin level in fetus as compared to mother • Oxygen dissociation curve of fetal red cells is shifted to left as compared to adult red cells.
Oxygen exchange function • HbF has less affinity towards organic phosphates like 2,3 DPG and ATP. • These phosphates that are present in red cells compete with oxygen for binding to hemoglobin. • Affinity of reduced hemoglobin to 2,3 DPG is higher than that of oxyhemoglobin and this facilitates oxygen delivery at tissue site.
Oxygen exchange function • CO2 crosses placenta from fetus to mother, it creates a local acidosis. • mothers hemoglobin shows less affinity towards Hb and oxygen release is enhanced[Bohr effect] • This supports diffusion of more oxygen across the diffusion membrane to fetus.
Umbilical vein to portal circulation • Some blood from the umbilical vein enters the portal circulation allowing the liver to process nutrients. • The majority of the blood enters the ductus venosus,.
Foramen ovale • Blood is shunted from right atrium to left atrium, skipping the lungs. • FO-Is a valve with two flaps that prevent back-flow.
Ductus arteriosus • The blood pumped from the right ventricle enters the pulmonary trunk. • Most of this blood is shunted into the aortic arch through the ductus arteriosus.
Fetal circulation physiology • Most of the unsaturated blood reaches the right ventricle- and this blood is channelled via the ductusarteriosus and descending aorta to the placenta for oxygenation • Most of the saturated blood reaches the left ventricle - driven into the ascending aorta to the heart and brain
How this is achieved? • By the appropriate mixing of the venous blood returning to the heart • And its preferential streaming
Central venous circulation • 5 sources: • upper body - SVC • myocardium – coronary sinus • the lungs – pulmonary veins • the lower body - IVC • placenta – umbilical vein ductus venosus IVC
Least saturated blood • From upper body via SVC • From myocardium via coronary sinus This blood is directed to the RV via the tricuspid valve
Venous return from lungs • Not well saturated • Preferential flow to RV is not possible • only 8% of combined ventricular output • So no appreciable effect on oxygen delivery
Inferior venacaval return • Lower body • Placenta
How this blood is preferentially directed to the RV • due to the leftward and superior course of the eustachian valve SVC blood is directed away from the foramen ovale and through the tricuspid valve • The location of the coronary sinus caudal to the foramen
How preferential flow occurs • Lower body flow except that from the liver ascends the distal IVC and this stream of relatively desaturated blood enters the lateral margin of the right atrium and directed to the RV via TV • Umbilical venous return to the LV • Venous flow from the liver – from right lobe to the RV and the left lobe to the LV via foramen ovale
Venous return to heart • Umbilical vein gives branches to left lobe of liver and then divides into DV and arcuate vein. • Arcuate vein joins the portal vein and then gives of branches to right lobe of liver. • Left hepatic vein joins the DV at it’s entry to IVC and Right hepatic vein joins the IVC directly.
Venous return to heart • Right lobe of liver receives poorly oxygenated portal venous blood and left lobe receives well oxygenated umbilical venous blood. • Both lobes receive small contribution of blood from hepatic artery. • Saturation of RHV is lower than that of LHV.
Venous return to heart • Posterior and left stream of IVC blood carries oxygenated blood while anterior and right stream carries poorly oxygenated blood. • Preferential streaming of DV and LHV blood across the foramen ovale and abdominal IVC and RHV blood across the TV.
Venous return to heart • Eustachian valve helps to direct the IVC blood to cross the foramen ovale. • The lower margin of septum secundum [crista dividens] helps to direct the left posterior stream to preferentially across the foramen ovale. • SVC blood is directed aross the TV.
Physiologic regulation of pulmonary vascular resistance • Pulmonary vascular resistance in the fetal lung is initially high • The most prominent factor associated with high fetal pulmonary vascular resistance is the normally low blood O2 tension (pulmonary arterial blood pO2 = 17 to 20 torr).
PVR in FETUS is high • all small pulmonary arteries have a thicker medial smooth muscle layer in relation to diameter • This increased muscularity is partly responsible for the increased vasoreactivity and pulmonary vascular resistance in the fetus
PULMONARY CIRCULATION • Experiments show fetal PBF increases dramatically in response to increase in maternal PO2. • This response is evident only in latter part of gestation. • Doppler studies indicate similar changes in humans as well.
Modulation of pulmonary vascular tone • Oxygen modulates the production of both prostacyclin and endothelium-derived nitric oxide (EDNO) • alpha agonists, thromboxane, and the leukotrienes are other mediators of increased pulmonary vascular tone
The combined ventricular output • the output of the two ventricles, and it also represents total venous return to the fetal heart. • The right ventricle ejects about 55-65%, and the left only 35-45% of CVO.
Cardiac output and its distribution • CVO is 450 ml/mt/kg • UV flow is 200 ml/mt/kg [45% of CVO] • Of this,110 ml/mt [24%] passes through DV and 90 ml/mt[21%] passes through hepatic circulation
Cardiac output and its distribution • Total venous return to heart from IVC is 315 ml/mt and represents 69% of CVO. • Of this 115 ml/mt [25% of CVO] passes through FO and and 200 ml/mt [44%] passes through TV.
Cardiac output in human fetus • Fetus increases the cardiac output by increasing the heart rate as it is incapable of increasing the stroke volume • Myocardium is underdeveloped • Fluid content is more • Myocardium surrounded by fluid filled lung
Blood oxygen saturations • The highest partial pressure of oxygen (Po2) is found in the umbilical vein (32 mm Hg) • The brain and coronary circulation receive blood with higher oxygen saturation (Po2 of 28 mm Hg) when compared to the saturation in the blood supply to the lower body (Po2 of 24)
The atrial and ventricular pressures • The wide communication at the atrial level (foramen ovale) allows for near equalization of atrial and ventricular end-diastolic pressures. • Similarly, at the great vessel level, the nonrestrictive ductus arteriosus allows equalization of systolic pressures