Download
1 / 13
180 likes | 1.16k Views
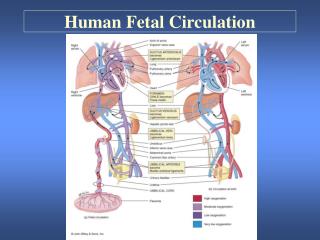
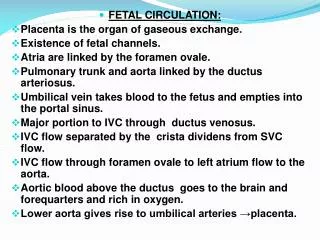
Fetal Circulation. Fetal Circulation: Overview. Fetal Circulation: Parturition. Uterine contractions squeeze head and body thereby expelling fluid from fetal lung. Subsequent contractions deliver the placenta thereby severing connection between fetal and maternal blood supply.

E N D
Fetal Circulation: Parturition • Uterine contractions squeeze head and body thereby expelling fluid from fetal lung. • Subsequent contractions deliver the placenta thereby severing connection between fetal and maternal blood supply. • During birthing process, placental capillaries are crushed, and thus the fetal systemic circuit’s resistance goes up almost 2 fold. (remember: placental circ. WAS about HALF of TOTAL fetal circ., thus removing this parallel circuit would DOUBLE resistance)
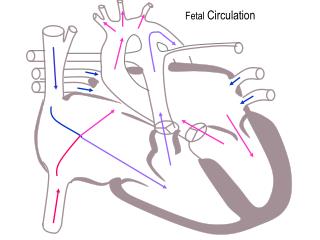
Fetal Circulation: Parturition Contd. • Assuming that CO remains the same, doubling resistance should also double the pressure within fetal circulation (by P=QR) • Also, another effect of increasing R is that this briefly DECREASES movement of blood into the IVC, which results in a decrease in RIGHT ATRIAL PRESSURE! • Now, pressure in LEFT atrium is higher than right, and so flow of blood through foramen ovale stops! (See pic to visualize this)
Fetal Circulation: Parturition Contd. • Flap of tissue in Left Heart covers up the Foramen Ovale. Now even LEFT to RIGHT blood flow (due to reversal of relative atrial pressure) cannot take place. • As a result, RV output can ONLY enter the pulmonary artery.
Fetal Circulation: First Breath • Post-birth, pO2 goes down while pCO2 goes up (this is new to the baby); this is sensed by chemorecs and initiates first breath. • Also, breathing may be influenced by gasps due to “startle reflex”. (baby is startled upon seeing new things etc…and so gasps, which helps with first breath too) • The loss of “immersion reflex” may influence breathing. (immersion reflex = if underwater, as in utero, drive to breathe goes down. Post birth, this inhibition is removed, thus baby tries to breathe)
Fetal Circulation: First Breath Contd. • Need to generate 80cm of water worth of pressure to establish alveolar liquid-air interface upon first breath. • Need to therefore decrease INTRATHORAIC (IT) pressure by a lot via contraction of diaphragm and external intercostals. • This decrease in IT pressure not only allows enough of a pressure gradient to breathe, but also elicits MAJOR changes in circulation.
Fetal Circulation: First Breath Contd. • When IT pressure is decreased, the pressure in lungs goes down too, SO…there is less pressure surrounding the pulmonary vessels as well (think about this…) • Because of this, there is now a greater difference in pressure between right ventricle (we didn’t do much to P here) and pulmonary vessels (P went down here). • This difference now allows for more blood to flow through these vessels since they are now more dilated
Fetal Circulation: First Breath Contd. • Now, vessels exhibit HIGH FLOW and LOW RESISTANCE properties characteristic of adult pulmonary circulation. • Also, since you are now oxygenating the alveoli, you release the hypoxia-induced vasoconstrictive tendencies which were predominant during fetal circulation.
Fetal Circulation: First Breath Contd. • As breathing continues, a greater % of blood from the RV enters the pulmonary circulation. • This increases FLOW to the LEFT ATRIUM, which causes an increase in LA pressure. (this increase in LA pressure also prevents movement of blood from RA to LA via a patent foramen ovale…critical because it prevents venous blood from mixing with arterial blood!!!)
Fetal Circulation: Ductus Arteriosus (DA) • Since blood flow through lung increases after birth, so does return of blood to the LA and, by extension, to the LV!!! • Increase in blood flow to LV, via STARLING FORCES, increases LV contractility. • This increases aortic systolic pressure. • Increase in aortic pressure prevents blood moving from RIGHT to LEFT into the DA (see pic!!!).
Fetal Circulation: Ductus Arteriosus (DA) • DA acts like other systemic vessels; that is, when introduced to high O2 environments, they CONSTRICT. • Thus, when pulmonary circulation improves after birth, P02 increases as well. Thus, the DA constricts!!! • Prostacyclins prevent the constriction of the DA. • One way to treat patent DA is to administer a prostacyclin synthesis inhibitor such as INDOMETHICIN.
Fetal Circulation: Ductus Arteriosus (DA) • LAST NOTE: During fetal circ, RV pressure is higher than LV pressure because of reasons already discussed (hypoxic vasoconstriction, we haven’t decreased IT pressure yet, fluid surrounding the lungs in utero etc…) • After birth, this all reverses such that LV pressure is greater than RV pressure. • You will therefore see a switch from a thick RV wall during fetal life to a thick LV wall during adult life. (ie. Wall thickness reflects pressure levels…since muscle grows in response to work…and work = PRESSURE * Volume)