Download
1 / 60
610 likes | 828 Views
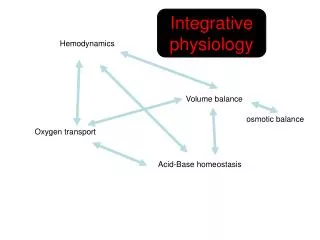
Quantitative Acid-Base Chemistry & Acid-Base Physiology (They are not the same). P Wilkes MD, PhD, FRCP University of Ottawa Heart Institute. Guiding Principles. Physiology will not violate the laws of chemistry and physics

E N D
Quantitative Acid-Base Chemistry & Acid-Base Physiology(They are not the same) P Wilkes MD, PhD, FRCP University of Ottawa Heart Institute
Guiding Principles Physiology will not violate the laws of chemistry and physics There is a difference between cause and effect vs. correlation (physics vs. math) In many ways – you do not know anything unless you know everything (If the devil is in the details – so is salvation)
Learning Objectives The Chemistry The Physiology The Clinical Approach
The ‘Chemistry’ in the Text Books‘The CO2 Hydration Reaction’ Chemical Description: CO2 + H20 H2CO3 HCO3- + H+ Mathematical Description, the Henderson-Hasselbalch equation: pH = pK + log [HCO3-] (.PCO2)
[HCO3-] PCO2=60 PCO2=40 30 24 14 Resp acidosis Metab alkalosis PCO2=30 Metab acidosis Resp alkalosis 7.0 7.4 7.6
PCO2=60 PCO2=40 30 24 14 Hg [HCO3-] PCO2=30 7.0 7.4 7.6 pH
BE = (1-0.014Hgb)(HCO3-24)+(1.43Hgb +7.7)(pH-7.4) PCO2=40 30 24 14 PCO2=30 [HCO3-] Base Excess Measured Decrease in [HCO3-] 7.0 7.4 7.6 pH
CO2 Hydration Reaction What is the pH of water equilibrated to PCO2 = 40 mmHg? ? 7.4 ? Higher ? Lower Answer 4.4 What is the HCO3? ? 24 mEq/L ? Higher ? Lower Answer < 1 mEq/L
What is Going On? The Problem: The CO2 hydration reaction does not predict what we measure in blood!! Nevertheless, the Henderson-Hasselbalch equation does?? The Answer: The CO2 hydration reaction is either wrong or incomplete
Modern Quantitative Acid – Base Chemistry(The Real Chemistry)Peter A Stewart Can J Physio Pharmacol 61: 1444 - 1461, 1983
Physical Chemistry of CO2 and Water At pH 7.4 (i.e. [H+] = 4x10-5 mEq/L) HCO3 = 24 mEq/L How do you account for electrical neutrality? Condition: PCO2 = 40 mmHg Equations:[H+][OH-] = K’w CO2(K1) = [HCO3-][H+] [HCO3-](K2) = [CO3=][H+] [H+] - [HCO3-] - [CO3=] - [OH-] = 0 Solving: [H+] = 0.036 mEq/L, pH = 4.44 !![HCO3-] = 0.036 mEq/L[CO3=] and [OH-] < 1 x 10-6 mEq/L [H+], [HCO3-], [CO3=], [OH-] are determined ONLY by PCO2 & Dissociation Constants
How to Make Bicarb ? NaOH = 5 NaOH = 20 NaOH = 40 Necessary Condition [fixed + charge] & PCO2
The Fixed Positive Charge and Other Acids • Plasma [Na+] + [K+] – [Cl-] 140 mEq/L + 4 mEq/L – 100 mEq/L ~ 44 mEq/L positive charge • This is the Strong Ion Difference (SID) • Other Acids ? Albumin Phosphate Albumin + Phosphate = [Atot] ~ Total Protein (g/L) x 0.25 = Atot (mEq/L)
The Chemically Complete Solution Multiple components CO2 hydration reaction Weak Acids (Blood is thicker than water) Electrical Neutrality Systems Approach: Solve All Equations Simultaneously Independent vs. Dependent Variables
Water dissociation equilibrium [H+] x [OH-] = K’w Weak acid dissociation equilibrium [H+] x [A-] = KA x [HA] Conservation of mass for “A” [HA] + [A-] = [ATOT] Bicarbonate ion formation equilibrium [H+] x [HCO3-] = KCx pCO2 Carbonate ion formation equilibrium [H+] x [CO32-] = K3x [HCO3-] Electrical neutrality [SID] + [H+] - [HCO3-] - [A-] - [CO32-] - [OH-] = 0 SID – HCO3 – [A-] ~0 Na + K – Cl – HCO3 ~ [A-] (Is this familiar?) [A-] is the anion gap
Only the whole set of six equations can explain the quantitative properties of the system, and permit evaluation of any of the dependent variables • No one of the six equations is more, or less, important than the others. All six are essential
Solve for [H+] and get a big wet kiss: Please put away all calculators, you have 30 seconds beginning now [H+]4+{KA+[SID]}[H+]3+{KA([SID]-[Atot])-(K1.CO2+K’w)}[H+]2-{KA(K1.CO2+K’w)+K2.K1.CO2}[H+]-KA.K2.K1.CO2= 0 A[X]4 + B[X]3 + C[X]2 + D[X] + E = 0
A Fourth Order Polynomial !?! DUOH !?! Now what do I do??
I know – Use a computer ! ? [H+]4+{KA+[44]}[H+]3+{KA([44]-[20])-(K1.40+K’w)}[H+]2-{KA(K1.40+K’w)+K2.K1.40}[H+]-KA.K2.K1.40= 0 [H+] = 3.98 x 10–8 -Log 3.98 x 10-8 = 7.4 Insert: SID = Na+K-Cl = 140 + 4 -100 = 44 mEq/LPCO2 = 40 mmHgTprot = 80 g/L = 20 mEq/L
Why Does the Henderson-Hasselbalch Equation Seem to Work? Water dissociation equilibrium [H+] x [OH-] = K’w Weak acid dissociation equilibrium [H+] x [A-] = KA x [HA] Conservation of mass for “A” [HA] + [A-] = [ATOT] (20 mEq/L) Bicarbonate ion formation equilibrium [H+] x [HCO3-] = KCx pCO2 (40 mmHg) Carbonate ion formation equilibrium [H+] x [CO32-] = K3x [HCO3-] Electrical neutrality [SID] (44 mEq/L) + [H+] - [HCO3-] - [A-] - [CO32-] - [OH-] = 0 [H+] is determined by SID, PCO2 and Atot [H+] = 3.98x10-8 Eq/L (pH=7.4) in all 6 equations only if SID=44 mEq/L, PCO2=40mmHg and Atot=20 mEq/L Therefore [HCO3] must be ~ 24 mM/L (math not chemistry)
ParadigmShift [H+] = 3.98 x 10-8 Eq/L (i.e. pH=7.4) AND HCO3 = 24 mmol/L because: SID = 44 mEq/L PCO2 = 40 mmHg Tprot = 80 g/L (~20 mEq/L) 1) [H+] and [HCO3] DO NOT INFLUENCE EACH OTHER 2) The CO2 hydration reaction: a) incomplete chemical description of the system b) predicts acid-base but does not offer a cause/effect explanation 3) You must understand normal acid-base before you can understand abnormal acid-base
Does the Equation Work? (Wilkes AJP:1998)
Independent vs. Dependent In Vitro In Vivo Independent PCO2 = ƒ(VCO2, VA) SID = ƒ(dIn/dOut, Vd), Na, Cl Atot = ƒ(dIn, dOut, Vd) CO2 Na+, Cl- Dependent H, HCO3, CO3, Prot, ProtH, OH (not functions of dIn, dOut or Vd) Protein
Summary Cause and Effect [H+] PCO2 [OH-] [H+] = ƒ([SID], PCO2, [Tprot]) A(X)4 + B(X)3 + C(X)2 + D(X) + E = 0 [HCO3-] [SID] [CO3=] [Tprot] [Prot.H] [Prot-]
Conceptual Consequences • The model predicts what we measure • H+ and HCO3 are both determined by chemistry IN PLASMA, NOT physiology • H+ and HCO3 are not determined by intake or loss – the kidney is irrelevant!! • What does physiology control? 1) The concentrations of Na, K, Cl and thus the strong ion difference 2) PCO2 3) Total weak acid concentration
Influence of [SID] [Na+] = 137 mEq/L [Na+] = 143 mEq/L [K+] = 4 mEq/L [K+] = 4 mEq/L [Cl-] = 105 mEq/L [Cl-] = 96 mEq/L [SID] = 36 mEq/L [SID] = 51 mEq/L PCO2 = 40 mmHg PCO2 = 40 mmHg[Tprot] = 80 g/L [Tprot] = 80 g/L pH = 7.29 pH = 7.51 [HCO3-] = 20 mEq/L [HCO3-] = 34 mEq/L[Prot-] = 16 mEq/L [Prot-] = 17 mEq/L
‘Electrolyte’ Acidosis Usually iatrogenic Assumed to be ‘benign’ However: • Gut hypoperfusion/Post Op N/V (Gan, Anesth.1999; Williams, Anesth Analg. 1999) • Impaired Renal Blood Flow, GFR (Wilcox, J Clin Invest, 1983) • Difficulty diagnosing Lactacidosis?
First Patient 74 yo male, 48 hrs post MI, on BIPAP S. aureus infection, osteomyolytis (by MRI for neck pain) vs. endocarditis (by ECHO) Mod MR, EF 50%, no inotropes, stable BP (No Swan) COPD, DM, Creat 173 7.29/42/80/20/-6.7 AG = 15 Are you worried ?
First Patient: Approach Electrolytes: Na = 132, K = 4.9, Cl = 102 SID = 34 mEq/L Total Protein: 64 g/L ~ 15 mEq/L Electrical Neutrality: SID – HCO3 – Prot- ~ 0 34 - 20 - 15 = -1 Lactate = 1.5 mEq/L Electrolyte based acidosis, low SID
SID and Acid-Base Very common cause of met acidosis Iatrogenic hyperchloremic metabolic acidosis How does this occur?
Normal Protein = 80 g.L-1 SID = 44 mEq.L-1 PCO2 = 40 mmHg pH = 7.42 [HCO3-] = 27 mmol.L-1 [Prot-] = 16.8 mEq.L-1 Low Protein = 40 g.L-1 SID = 44 mEq.L-1 PCO2 = 40 mmHg pH = 7.533 [HCO3-] = 35 mEq.L-1 [Prot-] = 8.7 mEq.L-1 Influence of Plasma Protein
Hypoproteinemic Metabolic Alkalosis Prot- Prot- HCO3 HCO3 Na Na Cl Cl
Hypoproteinemia Decrease in COP (Schupbach et al., Vox Sang 35:332, 1978; Zabala Ann Ital Chir LXIV 4:387, 1993) • Fluid Shifts/Retention • Glomerular Filtration Pressure Metabolic Alkalosis (McAuliffe et al., Am J Med 81:86, 1986)
Consequences of Hypoproteinemic Metabolic Alkalosis Hypoventilation (McAuliffe AJM, 1986) Hyperventilation ! (Rossing, J Lab Clin Med, 1988) Difficulty assessing acid-base status • Anion gap = (Na + K – Cl – HCO3-) = Prot- • Hides lactacidosis
Case #3: POD #1 2200 hr, Emergency CABG LV III, Inotropic support, IABP 105/60, 38/20, CI = 2.0, SVR = 1200 ABG = 7.45/40/155/29/-2.2 Anion gap = Na + K – Cl – HCO3 = 17 Are you concerned ?
Third Patient: Approach Step 1: Electrolytes and SID Na = 139 K = 3.5 Cl = 96 SID = 46 mEq/L Step 2: Total Protein = 40 g/L Convert to mEq/L: 40 g/L x 0.25 = 10 mEq/L
Third Patient: Approach Step 3: Electrical Neutrality SID – HCO3 – Prot- ~ 0 + 5 mEq/L 46.5 – 29 – 10 = 7.5 mEq/L Either: Lab variation (~ 2%) Unmeasured acid Lactate = 8 mEq/L (Type A) Dead gut on laparotomy
How does Stewart approach affect concept of Anion Gap ? AG SID Prot HCO3 Na Cl AG = Na+K-Cl-HC03 = [Prot-] = [A-] from [HA]Ka = [A-][H+][Atot] = [HA] + [A-] [A-] = KaAtot Ka+[H+] Therefore: AG can be measured directly
How does the Stewart approach affect concept of BE? From BE = (1-0.014Hgb)(HCO3-24)+(1.43Hgb +7.7)(pH-7.4) BE = 0 when pH = 7.4 and [HCO3] = 24 From Stewart: pH and [HCO3] are dependent upon prevailing PCO2, SID and Atot Therefore BE is also a function of PCO2, SID and Atot Atot and SID can both be altered by pathophysiology such that neither pH or HCO3 change Both Atot and SID should be assessed during a clinical evaluation
Information from BEBE = (1-0.014Hgb)(HCO3-24)+(1.43Hgb +7.7)(pH-7.4)HgB = 14 pH = 7.4 HCO3 = 24 PCO2 = 40 BE = 0 Na = 140 K = 4 Cl = 100 AG = 16 pH = 7.3 HCO3 = 16 PCO2 = 30 BE = -9.2 Na = 140 K = 4 Cl = 100 AG = 24 pH = 7.24 HCO3 = 16 PCO2 = 35 BE = -10.9 Na = 130 K = 4 Cl = 105 AG = 9 pH = 7.38 HCO3 = 25 PCO2 = 40 BE = +1.2 Na = 140 K = 4 Cl = 100 AG = 15 SID = 44 Tprot = 20 mEq/L SID-HCO3-TP~0 44 – 24 – 20 ~ 0 Lact = 10 SID = 44 (-10) Tprot = 20 mEq/L SID-HCO3-TP~0 34 – 16 – 20 = 2 SID = 29 Tprot = 15 SID-HCO3–TP~ 0 29 – 16 – 15 = -2 Lact = 0 SID = 44 Tprot = 10 mEq/L SID-HCO3-TP~10 44 – 25 – 10 = 9 Lact = 10
Model Summary SID (electrolyte or metabolic) acidosis SID (electrolyte) alkalosis Weak acid (protein) alkalosis (Weak acid (phos-, protein) acidosis) PCO2 acidosis PCO2 alkalosis
Compensatory Responses • Metabolic acidosis Hyperventilate Lower PCO2 • Metabolic alkalosis • 2nd low protein Decrease SID by increase Cl • 2nd increased SID Hypoventilate Increase PCO2 • Respiratory acidosis Increase SID by decreasing Cl • Respiratory alkalosis ?increase protein ?decrease SID
Respiratory Acidosis • Compensatory response to hypercapnea in severe COPD is to increase SID by lowering Cl (Alfero 1996)
The Law of Electrical NeutralityA Law of Physics – it ALWAYS exist SID + H+ - HCO3- - Prot- - Phos-- CO3= - OH- =0 SID – HCO3- - Prot- - Phos- ~ 0 {HCO3- + Prot- + Phos-} ~ SID {HCO3- - Prot- - Phos-} ~ {Na + Mg + Ca + K – Cl – Lact} What if electrical neutrality APPEARS not to exist?
Influence of Apparent Charge Imbalance[SID] - [HCO3-] - [Prot-] ~ 0(Wilkes, AJP, 1998) if UMI = 0, dpH = 0.0214