Download
1 / 40
400 likes | 549 Views
LOKALIZED FIBROUS TUMORS OF THE PLEURA. LOKALIZED FIBROUS TUMORS OF THE PLEURA. Dr. Refik ÜLKÜ Dicle University School of Medicine Thoracic Surgery Department. Dr. Refik ÜLKÜ Dicle University School of Medicine Thoracic Surgery Department.

E N D
LOKALIZED FIBROUS TUMORS OF THE PLEURA. LOKALIZED FIBROUS TUMORS OF THE PLEURA. Dr. Refik ÜLKÜ Dicle UniversitySchool of Medicine ThoracicSurgeryDepartment Dr. Refik ÜLKÜ Dicle UniversitySchool of Medicine ThoracicSurgeryDepartment
1767 Lieutauddescribedforthefirst time a primarytumor of thepleura • 1870 Wagner- describedPrimarylocalizedpleuraltumor • 1931-KlemperandRabin, publishedthefirstaccuratepathologicdescriptionandclassifiedmesothelioma as either ‘Localized’ or ‘diffuse’. • 1942- StoutandMurrayclaimedthatlocalizedmesothelioma had a mesothelialorigin. • Theotherstudies; Mesotheliallayercoveringthetumorwasintact. Epithelialcellsseencouldhavebeentrappedwithin growingfibrousmesenchymaltumors. AnnThoracSurg 2002; 74 :285-93 Int J Surgery 2008; 6: 298-301
The controversy on the origin of these tumors persisted for several decades and is reflected by thevariety of terms given to the neoplasm. • Localized mesothelioma • Localized fibrous mesothelioma • Localized fibrous tumors • Solitary fibrous mesothelioma • Fibrous mesothelioma • Pleural fibroma • Submesothelialfibroma • Subserosalfibroma AnnThoracSurg 2002; 74: 285-93
Recently, Localizedfibroustumorrecognized as nonmesothelial in orginandmesenchymalorigin.
Plevra tümörleri Diffüz Lökalize its associationwith asbestos(-) Goodoutcomes Etiology ? Solitarybenign its associationwith asbestos (+) Pooroutcomes (+)
Clinical Features • LFTP arerare. Theyaccountfor 5%- 10% allpleuralneoplasms. • Approximaely 900 cases of LFTP havebeenreported in theliterature. • LFTP areslow-growingneoplasms. • About 12 % of LFTP, however, aremalignantandeventuallyleadtodeaththroughlocalreccurenceormetastaticdisease. 1- ArchBronconeumol 2004; 40: 329-32 2- AnnThoracSurg 2002;74:285-93 3- AnnThoracSurg 2009; 88: 1632-7
LFTP havebeendescribed in allagegroupsfrom 5 to 87 years.(Chilhood time • Theypeak in thesixthandseventhdecades of life. • LFTP appearequalfrequency in men andwomen.. • LFTP is fortuitous in 50 % of cases. • Asymptomatic ( They can be asymptomatic 68 months on theavaregepriortoreferral.) • Preoperatifdiagnosis is extremelydifficultor not possible in manycases. 1- OncologyHematology 2003;47:29-33 2- EJSO 2005; 31: 84-87
Symptoms Asymptomatic (Themost of patients) ParaneoplasticSyndromes • Cough (%33%) • Chestpain (%23%) • Dyspnea (%19) • Obstructivepneumonitis • Hemoptysis Pierre-Marie-Bamberg syndrome Doege-PotterSyndrome
Digital clubbing and hypertrophic pulmonary osteoarthropathy(Pierre-Marie-Bamberg syndrome) have beendescribed in 10% to 20% of patients with either benign ormalignant LFTP • Hypoglisemiahavebeendescribed in 4% of patientswithlargetumor. • LFTP can also secrete insulin-like growth factorII, which causes refractory hypoglycemia (Doege-Pottersyndrome) • Hypoglisemiareturn tonormal values within 3 to 4 days after resection of thetumor
PLEURAL EFFUSION? • Pleuraleffusionaffects 16% of thepatients. • Malignanttumors: 32% • Benigntumors: 8 % • PE aregenerallysmall of a small size, althoughvolumes as great as 3 L havebeenreported in theliterature.
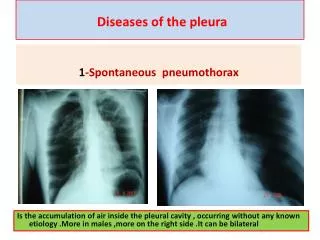
Chest radiograph: LFTP usually appear as a welldefined, homogeneous, and rounded mass. Rarely pleural effusion (+) Pedunculated SFTP have occasionally been reported to be moving on successive chest radiographs. CT: Well-delineated, homogeneous (smalllession), Heterogeneity ( hemorrhage, necrosis ) Softtissueattenuation, Tumors arising in an interlobar fissure may be more difficult to differentiatefrom an intraparenchymal mass. Calcification : (1/4 patient) Diffusepulmonarycollapseduetocompression (+)
MR MRI use in theassessment of pleural disease. The morphologyand relationship of LFTP to adjacent mediastinal ,major vascular structures anddiaphragmmay be betterappreciated with magnetic resonance imaging than withcomputed Tomography. LFTP haslow signal intensity on T1-T2 weighted images. Highsignalintensity: Increase vascularity, edemaandcellularity
PET-CT • Limitedapplicability • Tothemalignancyassessment: Highnegativepredictivevalue
Generally, 75/80% of tumors develops as a pedunculated growth from the visceral pleura. • In theremaining 20/25%developsfromparietalpleura. • LFTP with an origin from the parietal pleura and a sessilemorphology has more aggressive behavior.
The size of tumor ?prognosticfactor • In study of Perna, out of the 9tumors with benign histological features and 4 out of the 6tumors with malignant histological features were over 10 cmin diameter; They also classified a 23 cmtumor as benign, whichindicates that large size is not necessarily a marker ofmalignancy.
Some authors have observed that the size of the tumoris a prognostic factor for the clinical behavior of LFTP. • De Perrot observed that, all the patients reported with abenign tumor larger than 10 cm had a good clinicaloutcome, whereas 16 out of the 28 malignanttumorslarger than 10 cm were associated with recurrence ordeath.
CT guided aspiration biopsy is not a reliable diagnostictool. Cardillo et al. (2009)- 39% Magdeleinat et al. (2002)- 45% Kohler et al. ( 2007)- 40% 1-ArchBronconeumol 2004; 7: 329-32 2-Int J Surgery 2008; 6: 298-301 3-Eur J Cardiothorac Sur 2002; 21: 1087-93
Histopathology(1) • Benign SFTP are smallpedunculated tumors. • The malignant tumors are oftenlarger than 10 cm and grow beneath the parietal pleura ofthe chest wall, diaphragm, or mediastinum. Macroscopically: • Firm, smoothly lobulated masses (+) • Most of cases arecapsulated by a thin, translucent membrane, containing a reticulated vascular network. • Firm adhesion withoutsigns of invasion (+) • The cutsurface appears gray-whiteand may show areas of hemorrhage and necrosis.
Histopathology(2) Microscopically • SFTP are not characterized by uniformcell. • Proliferation of elongatespindlecell (+) • Zones of hypercellularity may alternate with hypocellular • Increasedamount of blood vessels within the tumor: Hemangiopericytoma-like pattern
SFTP are histologically characterized by fibrous areaswith low to moderate cellularity with spindle-shaped oroval cells scattered haphazardly among strands ofcollagen in a typical ‘‘patternless pattern.’’ J Surg Oncol 2006; 94: 40-4.
Immunohistochemistry has been an extremely usefultool to differentiate SFTP from mesotheliomas and othersarcomas over the last few years . • SFTPby definition is vimentinpositive and keratin,S-100negative. Inaddition, CD34 is positive in most benign and malignantSFTP. • The antiapoptoticprotooncogenebcl-2 is strongly expressed in SFTP. • Recently, some authors have demonstrated that(CD99) could be expressed by solitaryfibrous tumors located in the pleura
Over the last 20 years, immunohistochemical studies have provided strong evidence for a mesenchymal origin of these tumors. Vimentin (+) Keratin (-) CD34 (+) CD99 (+) bcl-2 (+)
Instudies of England and coworkers; • Therewere223 cases. • Eighty-twocases were describedas histologically malignant. • None of the patientswith a histologically benign disease died, 55% of thosewith a malignant form died because of recurrences ormetastases. • The authors observed complete resectability was the single mostimportant predictor of outcome.
De Perrotreviewed data of 185 patients. 19 (10%) of the patients presented at leastone recurrence of their tumor Of the 35 patients who presented arecurrence or died of the disease 27 had a primary sessiletumor with histologic sign of malignancy 5patientspresented with a primary sessile histologically benigntumor 2 with a primary pedunculatedhistologicallymalignant tumor. One patient with a pedunculatedhistologicallybenign tumor presented a recurrence (or anew primary tumor)
High mitoticcounts, defined as more than four mitoses per 10 highpowerfields • Mild to marked pleomorphism based on • nuclear size, irregularity, and nuclear prominence • Bundles of high cellularity with crowding and overlappingof nuclei, • Presence of necrotic or hemorrhagic zones; • Stromal or vascular invasion • Hafifilabelirgin nükleerpleomorfizm, • Nukleuslarınbirbirlerinekarıştığıartmışselülarite, • Nekrotikveyahemorajikalanlarınvarlığı • Stromalveyavaskülerinvazyon.
Classification of Solitary Fibrous Tumors of thePleura Ann ThoracSurg 2002; 74: 285-93
Treatment • Often it is impossible to make adefinite pre-operatory diagnosis for this tumor • The mainstay oftherapyen bloc surgical resection. • Thoracotomy diagnostic - therapeutictool. (A distance of1 to 2 cm from the tumor is usually recommended to bein healthy tissue.) • Generally, there is no lymph-node involvement • Thepedunculated tumors can besafely resected with a wedge resection of the lung. • In order to achieve complete resection in sessile tumorslobectomyor a pneumonectomy
Difficulties may arise during surgery due to the size ofthe tumor, to richly vascularized pleural adhesions andto a wide pedicle attaching the mass to the inside of thelung, the diaphragm, the mediastinum or the thoracicwall. • Someauthorsreportedcases of relapse 17-20 years after no radicalsurgery resection. • The relapsesaremore aggressive than the primary tumor.
Frozen section can be helpful to demonstrate that the resection margins are free of tumors, but this isnot routinely required. • Tumors adherent to the parietal pleura require anextrapleural dissection. • If the tumor denselyadheres to or invades the chest wall Chest wall resection
In 3% or less ofthe cases, the tumor can be “inverted” and grow insidethe lung parenchyma. These tumors may occasionallyrequire a lobectomy or a sleeve lobectomy. • Thoracoscopicapproaches : Itcan be safely used to removesmall pedunculated tumors located on the visceralpleura.(contact metastasis ?) • Some authors have also recommendedthe assistance of a video camera (video-assisted thoracicsurgery) to obtain a more precise view of the resectionmargins in some large, broad-based tumors of the parietalpleura
ADJUVANT TREATMENT • The role of adjuvant therapy in LFTP; ? (limited number ofpatients ) • Radio and chemotherapy haveshown to be effective in treating selected patients. • Afterradicalsurgery, Cardiolloneverrecommedeither RT and CT. • RT appearsto be indicatedonlywhensurgicalresectionincomplete.
Veronesi and colleagues, have observed significant reduction of an inoperablerecurrent SFTP with cyclofosfamide and adriamycin. • Neoadjuvant therapy could be helpful in large malignant tumors, its use is limited by the difficulty ofobtaining a precise preoperative diagnosis even with anopen biopsy
Conclusion: AlthoughLFTP are considered histologicallybenign tumors, because of the risk of recurrence and malignanttransformation, complete surgical resection is indicatedand long-term follow-up is recommended in all patients.