Download
1 / 31
310 likes | 415 Views
Clinical practice and safety in persistent pain management. Chris Herndon, PharmD Associate Professor Southern Illinois University Edwardsville. Disclosures. Nothing to disclose. Objectives .

E N D
Clinical practice and safety in persistent pain management Chris Herndon, PharmD Associate Professor Southern Illinois University Edwardsville
Disclosures • Nothing to disclose
Objectives • Define tolerance, addiction, hyperalgesia, misuse, abuse, diversion, and aberrant drug taking behaviors • Describe the risks versus benefits of opioid therapy in the treatment of persistent noncancer pain • Identify methods for stratifying risk of misuse among patients with chronic pain • Develop monitoring strategies for patients requiring chronic opioid therapy based on risk level
Important Definitions • Dependence • Addiction (substance abuse disorder) • Aberrant drug taking behavior • Misuse • Abuse • Diversion • Tolerance • Pseudo-addiction (oligo-analgesia) • Hyperalgesia
The Challenge in Treatment Untreated or undertreated pain Overdose, abuse, diversion
Important Definitions • Dependence a physiologic, receptor response to an exogenous substance and the result from removing that substance • Addiction (substance abuse disorder) • Aberrant drug taking behavior • Misuse • Abuse • Diversion • Tolerance • Pseudo-addiction (oligo-analgesia) • Hyperalgesia
Important Definitions • Dependence • Addiction (substance abuse disorder) Impaired control over drug use, compulsive use, continued use despite harm, cravings • Aberrant drug taking behavior • Misuse • Abuse • Diversion • Tolerance • Pseudo-addiction (oligo-analgesia) • Hyperalgesia
Important Definitions • Dependence • Addiction (substance abuse disorder) • Aberrant drug taking behavior Any drug-related behaviors other than taking the med exactly as prescribed • Misuse • Abuse • Diversion • Tolerance • Pseudo-addiction (oligo-analgesia) • Hyperalgesia
Important Definitions • Dependence • Addiction (substance abuse disorder) • Aberrant drug taking behavior • Misuse • The use of a medication, FOR THERAPEUTIC INTENT, other than exactly as directed by the prescriber • Abuse • Diversion • Tolerance • Pseudo-addiction (oligo-analgesia) • Hyperalgesia
Important Definitions • Dependence • Addiction (substance abuse disorder) • Aberrant drug taking behavior • Misuse • Abuse The use of a substance for a non-medical purpose to alter one’s state of conciousness • Diversion • Tolerance • Pseudo-addiction (oligo-analgesia) • Hyperalgesia
Important Definitions • Dependence • Addiction (substance abuse disorder) • Aberrant drug taking behavior • Misuse • Abuse • Diversion Knowingly transferring a controlled substance to a recipient other than for whom the substance is prescribed • Tolerance • Pseudo-addiction (oligo-analgesia) • Hyperalgesia
Important Definitions • Dependence • Addiction (substance abuse disorder) • Aberrant drug taking behavior • Misuse • Abuse • Diversion • Tolerance A state of pharmacological adaptation to a drug in which either efficacy or side effects diminish over time and higher doses are required to maintain effect • Pseudo-addiction (oligo-analgesia) • Hyperalgesia
Important Definitions • Dependence • Addiction (substance abuse disorder) • Aberrant drug taking behavior • Misuse • Abuse • Diversion • Tolerance • Pseudo-addiction (oligo-analgesia) exhibiting aberrant or addicted behaviors due to undertreatment of a legitimate pain syndrome • Hyperalgesia
Important Definitions • Dependence • Addiction (substance abuse disorder) • Aberrant drug taking behavior • Misuse • Abuse • Diversion • Tolerance • Pseudo-addiction (oligo-analgesia) • Hyperalgesia A phenomenon in which stimuli that hurt induce a response greater than expected. Opioid-induced hyperalgesia is represented by a worsening of pain with escalation of dose Webster LR, Fine PG. Approaches to improve pain relief while minimizing abuse liability. J Pain 2010; 11(7):602-611.
Guidelines on opioid use Chou R, et al. Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain. J Pain 2009;10(2):113-130. American Geriatrics Society. Pharmacologic management of persistent pain in older persons. J Am GeriatrSoc 2009;57:1331-1346. Trescot AM, et al. Opioids in the management of chronic non-cancer pain: An update of American Society of Interventional Pain Physicians’ Guidelines. Pain Physician 2008;11(2 Suppl):S5-S62.
Cochrane Systematic Review:Long-term opioid management for chronic noncancer pain Noble M, Treadwell JR, Tregear SJ, Coates VH, Wiffen PJ, Akafomo C, Schoelles KM. Long-term opioid management for chronic noncancer pain. Cochrane Database of Systematic Reviews 2010, Issue 1. Art. No.: CD006605. DOI: 10.1002/14651858.CD006605.pub2
What is considered “high dose” Walker JM, et al. Chronic opioid use is a risk factor for the development of central sleep apnea and ataxic breathing. J Clin Sleep Med 2007;3(5):455-461.
How and what should we monitor (inpatient)? • Opioid induced sedation • Ramsay • Pasero Opioid-Induced Sedation Scale (POSS) • Respiratory depression • Respiratory rate < 8? 10? • Continuous pulse-oximetry • End-tidal capnography Jarzyna D, et al. American Society for Pain Management Nursing guidelines on monitoring for opioid-induced sedation and respiratory depression. Pain Management Nursing 2011;12(3):118-145.
Validated Risk Assessment Tools α - SOAPP®-R (Screener and Opioid Assessment for Patient’s in Pain-revised); DIRE (Diagnosis, Intractability, Risk, and Efficacy); ORT (Webster’s Opioid Risk Tool); COMM (Current Opioid Misuse Measure); CAGE (Cut-down, Annoyed, Guilt, Eye-opener); PDUQ (Prescription Drug Use Questionnaire); STAR (Screening Tool for Addiction Risk); SISAP (Screening Instrument for Substance Abuse Potential); PMQ (Pain Medication Questionnaire)
Example of common screening toolOpioid Risk Tool Low Risk 0 – 3 points, Moderate Risk 4 – 7 points, High Risk > 8 points Webster LR, Webster RM. Predicting aberrant behaviors in opioid treated patients. Pain Med 2005;6(6)432-42.
Drug Testing • Biological specimens • Urine, blood, hair, saliva, sweat, and nails • All have different specificity and sensitivity • Urine mostly preferred • Ease of collection • Possibly higher drug concentrations and longer detection window
Urine Drug Screen • Immunoassay • Most commonly used • Disadvantage – false positives • Gas chromatography – mass spectrometry (GC –MS) • Confirmatory test for specific drug • More sensitive and reliable • Disadvantage - Cost * Know which test your institution uses are what compounds are being tested
Length Detection Time in Urine Moeller KE, Lee KC, Kissack JC. Urine drug screening: practical guide for clinicians. Mayo Clin Proc. 2008;83(1): 66-76.
Achieving SafeUse While Improving Patient Care Presented by CO*RE Collaboration for REMS Education www.core-rems.org Presented by CO*RE Collaboration for REMS Education www.corerems.org Collaborative for REMS Education
Patient Counseling DocumentRequired for CR / LA REMS • DO • Read the med guide • Take exactly as prescribed • Flush unused meds down toilet • Call healthcare provider for med advise or SE • DON’T • Give your medicine to others • Take medicine unless prescribed for you • Stop taking your medicine without direction • Break, chew, crush, dissolve, or inject your medicine • Drink alcohol while taking this medicine http://www.er-la-opioidrems.com/IwgUI/rems/pdf/patient_counseling_document.pdf. Accessed 10/12/12.
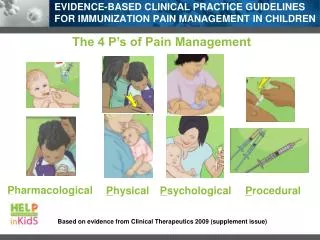
Appropriate Documentation • The 4 “As” of pain management • Analgesia • Adverse effects • Aberrant drug taking behavior • Activity • Diagnosis, prognosis, and correlation of symptoms
Pathways for primary care VAS: visual analog scale; NRS: numeric rating scale; BPI: Brief Pain Inventory; MPQ: McGill Pain Questionnaire; NPRS: Neuropathic Pain Rating Scale