Download
1 / 15
160 likes | 490 Views
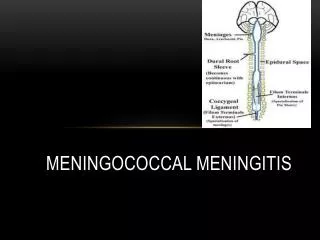
MENINGOCOCCAL DISEASE. EPIDEMIOLOGY 1. Meningococcal diseases are caused by Neisseria meningitidis. Encapsulated Gram negative diplococcus presently found only in human sources.

E N D
MENINGOCOCCAL DISEASE DR (MRS) M.B. FETUGA
EPIDEMIOLOGY 1 • Meningococcal diseases are caused by Neisseria meningitidis. • Encapsulated Gram negative diplococcus presently found only in human sources. • Grouped into serotypes using the capsular polysaccharide antigens but only types A, C, Y and W135 cause most infections. • Most meningococcal diseases in the developing world are caused by group A compared to B and C in the US. DR (MRS) M.B. FETUGA
EPIDEMIOLOGY 2 • Most cases occur in infancy. • NB infants have maternally-acquired protective AB. • Higher incidence among males. • Transmission is thro’ droplets from cases or carriers. • Overcrowding favours transmission. • About 10% of healthy children carry the organism at one time or the other in the nasopharynx. DR (MRS) M.B. FETUGA
EPIDEMIOLOGY 3 • The disease is endemic in most parts of the developing world but sporadic cases also occur. • Epidemics occur in the meningitis belt of Sub-Saharan Africa usually at the beginning of the dry season. These are usually caused by the serotypes A, C and W135. • Meningitidis is acquired by a respiratory route. Colonization of the nasopharynx usually leads to asymptomatic carriage, and only rarely does dissemination occur. Colonization can persist for weeks to months. DR (MRS) M.B. FETUGA
PATHOGENESIS • Organism produces proteases which destroy secretory IgA allowing colonization of the nasopharynx. • Dissemination from the URTI thro the bloodstream. • Most adults have developed natural immunity against N. meningitidis from nasopharyngeal colonization. Carriage of nonpathogenic N. lactamica , leads to the development of bactericidal AB against the meningococcus. • Individuals with primary or acquired complement deficiency (agammaglobulinaemia, SCA, SLE, Nephrotic syndrome) have an ↑ risk of developing meningococcal disease. DR (MRS) M.B. FETUGA
PATHOLOGY • Interaction of endotoxin released by N. meningitidis and the complement system probably → Complement activation → stimulation of monocytes and macrophages → production of cytokines (Interleukins and TNF-alpha) → activation of the fibrinolytic system → SYSTEMIC INFLAMMATORY RESPONSE (DIC, multiple organ system failure, septic shock, and death). DR (MRS) M.B. FETUGA
CLINICAL FEATURES 1 • Wide spectrum of meningococcal disease • Recognized patterns include: • Bacteremia without sepsis • Meningococcemia without meningitis • Meningitis with or without meningococcemia • Meningococcal infection of specific organs. • Bacteremia commonly presents with fever with or without URTI or diarrhoea which may be erroneously ignored. Spontaneous recovery without antibiotics may occur & it may progress to meningitis without antibiotics. DR (MRS) M.B. FETUGA
CLINICAL FEATURES 2 • Acute meningococcemia initially can mimic a virus-like illness with pharyngitis, fever, myalgias, weakness, and headache. With widespread hematogenous dissemination, the disease rapidly progresses to septic shock, adrenal hemorrhage, renal failure, myocardial failure, and coma. Meningitis may or may not develop. • Skin lesions include petechiae and/or purpura. Purpura fulminans may also develop in a few cases. DR (MRS) M.B. FETUGA
CLINICAL FEATURES 3 • Death usually follows within a few hours of onset. Xteristic finding on PM is massive bilateral adrenal haemorrhage (Waterhouse-Friderichsen syndrome). • Survivors have extensive ecchymosis with skin and muscle necrosis. Uncommon manifestations of meningococcal disease include endocarditis, purulent pericarditis, pneumonia, septic arthritis, endophthalmitis, periorbital cellulitis, mesenteric lymphadenitis, and osteomyelitis. DR (MRS) M.B. FETUGA
CLINICAL FEATURES 4 • Meningitis may also occur. Onset is shorter and seizures and focal neurologic signs occur less frequently than in pneumococcal or haemophilus meningitis. It usually responds to appropriate antibiotics and supportive therapy. • Chronic meningococcemia is very rare. Xterised by recurring fever, fleeting petechial or macular rashes. Response to antibiotics is also good. DR (MRS) M.B. FETUGA
DIAGNOSIS 1 • Definitive diagnosis of meningococcal disease is made by isolation of the organism from a either blood, CSF, or synovial fluid. • Culture or Gram stain of petechial or papular lesions has been variably successful in identifying meningococci. • Bacteria can occasionally be seen on Gram stain of the buffy coat layer of a spun blood sample. DR (MRS) M.B. FETUGA
DIAGNOSIS 2 • In meningitis, the morphologic and clinical characteristics of CSF are those of acute bacterial meningitis. • Latex agglutination & counterimmunoelectrophoresis can detect meningococcal capsular polysaccharide in CSF, serum, joint fluid, or urine. • Others include ↑ ESR and C-reactive protein, leukocytopenia or leukocytosis, thrombocytopenia, proteinuria, and hematuria. Patients with DIC have decreased serum concentrations of prothrombin and fibrinogen. DR (MRS) M.B. FETUGA
DIFFERENTIAL DIAGNOSIS • Measles (especially the haemorrhagic type) • Rubella • Gram negative septicaemia • Enteroviral (Echovirus & Coxsackie) infection • Idiopathic Thrombocytopenic Purpura • Drug reaction with erythema multiforme or erythema nodosum • Leptospirosis • Acute hemorrhagic encephalitis • Serum sickness • Henoch-Schonlein purpura • Kawasaki disease DR (MRS) M.B. FETUGA
TREATMENT • Crystalline Penicillin is the drug of choice and should be given intravenously in doses of 250,000–300,000 U/kg/24 hr for 7 days. • Ceftriaxone (100 mg/kg/24 hr), cefotaxime (200 mg/kg/24 hr) and chloramphenicol (100 mg/kg/24 hr IV in four divided doses) are useful alternatives. • Other supportive therapies are given as necesssary. DR (MRS) M.B. FETUGA
PREVENTION • Close contacts of patients with meningococcal disease as well as the household, daycare and school contacts should have the chemoprophylaxis. • Rifampin is given (10 mg/kg) orally every 12 hr for 2 days (total of four doses). Single doses of ceftriaxone and ciprofloxacin are also useful as prophylaxis. • A quadrivalent vaccine composed of capsular polysaccharide of meningococcal groups A, C, Y, and W135 is available. The immunogenicity of the vaccine in children younger than 2 years of age is unreliable but the introduction of the conjugate form of the vaccine has made it useful in all ages. Routine immunization of Nigerian children is recommended but has not been commenced. DR (MRS) M.B. FETUGA