Download
1 / 36
400 likes | 663 Views
meningococcal disease and vaccination. CME/CNE October 2011 Public Health Unit/Immunisation Advisory Centre, University of Auckland. Meningococcal C disease. Northland DHB disease outbreak and the meningococcal C vaccine. What this presentation covers.

E N D
meningococcal disease and vaccination CME/CNE October 2011 Public Health Unit/Immunisation Advisory Centre, University of Auckland
Meningococcal C disease Northland DHB disease outbreak and the meningococcal C vaccine
What this presentation covers • Meningococcal disease and meningitis • Symptoms and diagnosis • How you catch it • Types of meningococcal disease • Meningococcal disease – around the world • Protection against meningococcal disease • Meningococcal vaccine • Common questions
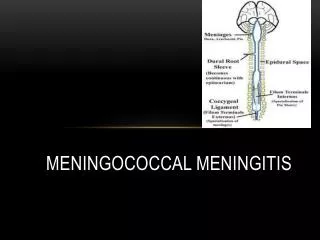
Meningococcal Disease • What it is • Symptoms • How you catch it
Meningococcal disease • Caused by Neisseria meningitidis • Frequently rapid onset • Bacteria in the bloodstream interferes with normal functions, leading to: • Blood poisoning (septicaemia) • Meningitis (Inflammation around the brain) • There is ~20% risk of permanent damage in survivors • Risk of death around 2-15% of cases • Depends on age, deprivation, early treatment, strain and presentation
Meningitis is also caused by other bugs • Meningitis caused by viruses • Usually less severe • Many causes e.g. mumps • Meningitis caused by bacteria • Usually more severe • Major causes in children • Hib (immunised against) • Pneumococcal (most common types immunised against) • Meningococcal
Early symptoms and diagnosis • Symptoms can vary a lot • Unwell, rash, headache, ‘flu-ish’ • Can change very quickly (hours) • Important to get rapid treatment • Early antibiotics can kill the bacteria quickly
Where meningococci lives • Lives in the nasopharynx (nose and throat) • Can be in the nose/throat for weeks to months (carriage) • Usually cleared by your immune system without getting sick • Occasionally it gets inside the bloodstream and causes the disease Thomas MG. New Zealand Medical Journal (2004) 117:1200.
How you catch it • Directly from another person • Commonly carried in the throat and back of nose (especially teenagers) • Droplets are spread from the nose and throat • Disease most often occurs in • Children under 3 years • Adolescents 15 – 18 years
Risk factors for meningococcal disease • Crowded living conditions, e.g. home or hostel • Recent respiratory infection • Exposure to cigarette smoke • Poor nutrition • Inherited (genetic) factors
meningococcal disease • Neisseriameningitidis
Types of meningococcal disease • Major ones are named A, B, C, Y, W-135 • Differ by their exterior sugar coat • The frequency of different types differs from country to country • NZ currently major types – B and C • Is in the community all the time in low numbers • Occasional outbreaks Men C Men B
History of meningococcal disease in NZ NZ ‘B’ ‘Auckland ‘A’
Northland from July 2011 • Recent increase in meningococcal disease • July-Sept • Nine confirmed cases • Children aged >1 to < 20 years, one elderly woman • Seven were Group C • Three deaths (all Group C) • This constitutes a community outbreak
Rate of meningococcal disease per 100,000 people under 20 years of age July-Sept 2011 Outbreak threshold
Northland meningococcal disease, number of cases in people between 1 and 20 years. 2005 – Sept 2011 Up to September
What protects against getting meningococcal disease? • Naturally acquired immunity • Artificially acquired immunity
Antibodies are very important • Specific antibodies present in the blood can neutralise the meningococci and bring about their destruction • Many studies have demonstrated that these antibodies are vital to prevent disease occurring • Three ways to get the antibodies • Transferred to fetus from mother (temporary) • Carriage • Vaccine
What about maternal protection? • Babies get protection from mother • Mostly through the placenta • Less through breast milk • Mostly gone by 6 months of age • Varies depending on woman (needs to have the protection herself in the first place)
Protection by vaccination • Antigens in the vaccine teach your immune system how to make specific antibodies • Depending on the vaccine, your immune system creates a memory for how to make those antibodies for a long time
Antibodies against the polysaccharide coat are very important Macrophages Polysaccharide coat Antibodies Meningococci C Meningococci B
Meningococcal C Conjugate Vaccine • Components • Effectiveness • Duration of protection
About the vaccine • Contains the meningococcal ‘C’ sugar (polysaccharide) attached to a protein • The protein stimulates the immune system to make antibodies and long-lasting memory • The vaccine also contains a tiny bit of aluminium salt (0.125mg) which assists in the immune response • NaCl (salt) • Sterile water
Countries using Meningitec® • Europe: • UK (on the NIS since 1999), France, Italy, Germany, Spain, Portugal, Ireland, Greece, Belgium, Switzerland, Hungary, Poland • Other countries: • Australia (on the NIS since 2003), Canada, Brazil, Hong Kong, Singapore
Measuring vaccine usefulness • Immunogenicity- immune response to vaccine • Efficacy- how well the vaccine did in (clinical) research trials • Effectiveness- effect of the vaccine on the disease in the real world
Meningococcal C conjugate vaccine • Immunogenicity/efficacy: 90% to 100% • Effectiveness e.g. reduction of disease by 95% in vaccinated population (UK) • 1998, 556 cases under 20 years • 2003, 29 cases under 20 years
Laboratory confirmed cases of meningococcal disease in England, 1998 - 2003 Vaccine introduced 1999 Centre for Infections. London: Health Protection Agency Centre for Infections. May 2005.
Duration of protection • Several years in younger children • Longer with older children, at least five years • If the disease returns in the community can vaccinate to boost protection Vaccination is important for both individual protection and community immunity (via reducing carriage)
Vaccine reactions Selected results from combined clinical trials Ongoing safety monitoring shows a very rare rate (less than 0.01%) for serious adverse reactions
Serious events • Fainting (a reaction to having an injection) • Anaphylactic reaction – extremely rare, 1/500,000 doses • Other adverse events occurring after receipt of this vaccine have been at the same rates as people who have not received the vaccine Andrews N, Stowe J, Miller E, Taylor B. Post-Licensure Safety of the Meningococcal Group C Conjugate Vaccine. Human vaccines. 2007;3(2):59-63.
For the Northland outbreak • 1 dose for all 1 year to under 20 years • intramuscular in the upper arm (or leg in young infants not yet weight bearing, usually under 15 months) • Why not give to infants under 1 year • No disease currently in under ones • Infants usually don’t carry it in their throat • Vaccine not effective for under ones in a single dose • Infants should get protection from less people carrying it
Summary: Key points • There are many different sorts of meningitis • There are different sorts of meningococcal disease • Be very aware of signs and ask for help early • There is currently an outbreak of Group C in Northland • There is a vaccine that is very effective in most children • International vaccine, used widely • Single dose in children 1 – 19 years • This vaccine works both for protection to the individual and reduces the spread in the whole community by reducing carriage in the throat • This vaccine has an excellent safety profile
Contacts • 0800 IMMUNE (466863) • Free phone line staffed by registered nurses with specialist expertise in vaccines and vaccine preventable diseases • Backed up by doctors and scientists • www.immune.org.nz • University of Auckland, Immunisation Advisory Centre website • Lots of links to other websites