Download
1 / 17
170 likes | 186 Views
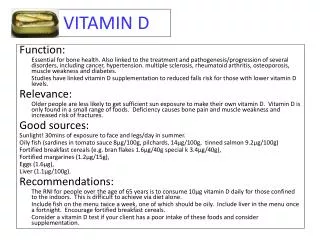
This review delves into recent trials and analyses on the effectiveness of Vitamin D supplementation for respiratory tract infections, asthma, and other related conditions. From bolus dosing to daily intake, the evidence points to varying outcomes, highlighting the importance of Vitamin D levels in determining efficacy.

E N D
Vitamin D: current state of the evidence John Hickner, MD, MS Editor-in-Chief, Journal of Family Practice
Objective Review recent randomized trials and meta-analyses describing the conditions for which Vitamin D supplementation is effective, ineffective or of unknown effectiveness.
Respiratory Tract Infections 1. Bolus dosing of Vitamin D does not prevent ARTI or asthma exacerbation in vitamin D–deficient patients • RCT: 590 patients with asthma, all using inhaled steroids • 120,000 IU Vit D q2 month or not • 82% had low vitD levels less than 30 ng/ml • No effect on exacerbations 2. Vitamin D does not reduce URIs in children age one to five • RCT: 703 children given either 2,000 IU daily or 400 IU daily • Mean of 1.05 ARI vs 1.03 in low dose group • No difference in any of the other outcomes • Flaw: both groups probably had adequate VitD levels
Respiratory Tract Infections 3. No effect of Vitamin D3 supplementation on respiratory tract infections in healthy individuals • 2016 systematic review: 15 RCTs with 7053 individuals • 6% risk reduction (RR 0.94); not statistically significant • Overall study quality rated as low 4. Vitamin D reduces the frequency of respiratory tract infections • 2017 systematic review: 25 RCTs with 11,321 individuals • Overall odds ratio of 0.88 favoring Vit D • Not effective if given as bolus dosing q month or longer • Best effect for those with low Vit D (less than 25). OR 0.3
Wheezing, asthma, COPD 5. Vitamin D supplementation during pregnancy does not prevent wheezing in the infant • RCT 623 Danish women: 2,400 IU vs 400 IU Vit D • 3 year follow up • No diff in wheezing, dx of asthma, eczema, URI 6. Prenatal vitamin D supplementation reduces risk of asthma/recurrent wheeze in early childhood • 1,387 women in 2 RCTs combined: 2400 IU or 4000 IU vs 400 • 26% risk reduction in asthma/wheezing by age 3 years • More effective if low vit D level • 6 year follow up shows no effect, however (JAMA 2019 Mar 12;321(10):1003-1005)
Wheezing, asthma, COPD 7. Vitamin D reduces the risk of asthma exacerbations requiring systemic steroids • Meta-analysis 8 studies, 1078 patients • 26% risk reduction in steroid requiring exacerbations; best in those with low Vit D levels: 67% relative risk reduction • No difference in overall exacerbations, however 8. Vitamin D reduced COPD exacerbations in patients with low vitamin D levels • Meta-analysis of 4 studies, 560 patients • Reduced risk only in those with low Vit D levels (RR: =0.55)
Pain 9. Vitamin D does not reduce pain in adults with symptomatic knee arthritis • RCT: 413 adults (340 completed study): 50,000 IU Vit D month for 2 years • Pain scores and cartilage volume same in both groups 10. Maintaining Vitamin D sufficiency Is associated with improved structural and symptomatic outcomes in knee osteoarthritis • Same study as 9 • Those with consistently higher vit D levels had somewhat better outcomes, suggesting Vit D MAY have some value • Biased analysis; needs confirmation
Pain 11. Vitamin D for the treatment of chronic painful conditions in adults • 2015 Cochrane review: 10 studies with 810 participants • Inconsistent results; now quality; need better evidence 12. Vitamin D supplementation improves pain symptoms in patients with chronic widespread pain/fibromyalgia • 4 RCTs with 286 participants • Mean difference of 0.46 on a 10 point visual analog scale • But no correlation between Vit D levels and pain relief
Fatigue and mental health 13. Vitamin D did not improve fatigue • 120 adults with fatigue and low Vit D but no diagnosed mental health condition; 50 point fatigue scale • RCT: Single large dose of Vit D: 100,000 IU or placebo • One month later, decrease 3.3 in Vit D group vs 0.8 in placebo • Statistically significant decline but not clinically meaningful diff. 14. Vitamin D does not improve symptoms of bipolar disorder • RCT: 5,000 IU Vit D vs. placebo for 12 weeks • Slightly better MADRS score (diff 3 points on 60 point scale) but no other differences
Depression (not in syllabus) • MAYBE according to one meta-analysis: Vellekkatt F, Menon V. Efficacy of vitamin D supplementation in major depression: A meta-analysis of randomized controlled trials. J Postgrad Med. 2018, Jun 21. • NOT EFFECTIVE in recent randomized trial: Hansen JP, Pareek M, Hvolby A, Schmedes A, Toft T, Dahl E, Nielsen CT. Vitamin D3 supplementation and treatment outcomes in patients with depression. BMC Res Notes. 2019 Apr 3;12(1):203.
Cardiovascular disease and cancer 15. High dose bolus Vitamin D does NOT prevent cardiovascular disease • RCT: 5110 participants from New Zealand • 200,000 IU, then 100,000 IU Vit D/month for avg 3.3 years • CV events 11.8% vs 11.5% in placebo group • No benefit, even for those with low Vit D level 16. Vitamin D plus calcium does not reduce cancer risk in postmenopausal women • RCT: 2303; Vit D 2000 IU QD and calcium 500 mg tid • 4 year follow-up: 3.89% vs 5.58%, favoring intervention, but not statistically significant and underpowered
Cardiovascular disease and cancer 17. No effect of Vitamin D on cancer mortality: meta-analysis • 2018 meta-analysis of 30 RCTs with 18,808 participants • No statistical diff in cancer rates or cancer deaths 18/19. Vitamin D supplements and prevention of cancer and cardiovascular disease • Large RCT of 25,871 participants • Vit D 2,000 IU and omega 3 fatty acid 1gm daily • Mean 5.3 year follow up: no statistically significant difference in any of many cancer and CV outcomes, including death
Diabetes 20. The Effect of Improved Serum 25-Hydroxyvitamin D Status on Glycemic Control in Diabetic Patients: A Meta-Analysis • 2017 meta-analysis • 24 controlled trials (1528 individuals diagnosed with type 2 diabetes • Small positive effect on A1c: 0.3% lower • Clinical significance not measured
What is a normal Vitamin D level? 21. Serum 25-Hydroxyvitamin D insufficiency in search of a bone disease • Cohort of 11,855 individuals in Australia • No biochemical abnormalities in bone metabolism (PTH, calcium, alkaline phosphotase) above a 25(OH) Vit D level of 12 ng/ml • Raises question about the current thresholds of 20 ng/ml for deficiency and 30 for insufficiency
What is a normal Vitamin D level? “A common misconception is that the RDA functions as a “cut-point” and that nearly the entire population must have a serum 25(OH)D level above 20 ng per milliliter to achieve good bone health. The reality is that the majority (about 97.5%) of the population has a requirement of 20 ng per milliliter or less.” • Manson JE, Brannon PM, Rosen CJ, Taylor CL. Vitamin D Deficiency - Is There Really a Pandemic? N Engl J Med. 2016 Nov 10;375(19):1817-1820.
Bottom Lines 1. Vitamin D modestly decreases frequency of acute respiratory infections. 2. Vitamin D decreases asthma exacerbations requiring steroids but not the rate of exacerbations. 3. Vitamin D reduces the frequency of moderate/severe COPD exacerbations in Vitamin D deficient individuals. 4. Vitamin D does not reduce pain from knee arthritis but does decrease the pain of chronic widespread pain syndrome.
Bottom Lines 5. Vitamin D does not decrease fatigue in otherwise normal individuals and is not effective for bipolar disorder, and probably not depression, but the jury is out on depression. 6. Vitamin D decreases A1C in type 2 diabetes; the clinical significance is unknown. 7. Vitamin D does not decrease the incidence of cardiovascular disease or cancers. 8. Current laboratory ranges for normal vitamin D levels are probably inaccurately high